NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Melanoma is a type of skin cancer that develops in melanocytes, the cells responsible for producing melanin. It is considered the most serious form of skin cancer because it can spread to other parts of the body if not detected and treated early. It typically occurs in the skin, but may rarely occur in the mouth, intestines, or eye. In women, melanomas most commonly occur on the legs, while in men, the back is the most common site.
The latest validated figures from the National Cancer Registry of Ireland (NCRI) in 2021 (Table 1) show 1,263 invasive melanomas were diagnosed in Ireland, confirming that melanoma is now the fourth most commonly diagnosed cancer in both men and women, and one in 38 of the population may develop a melanoma (www.ncri.ie).
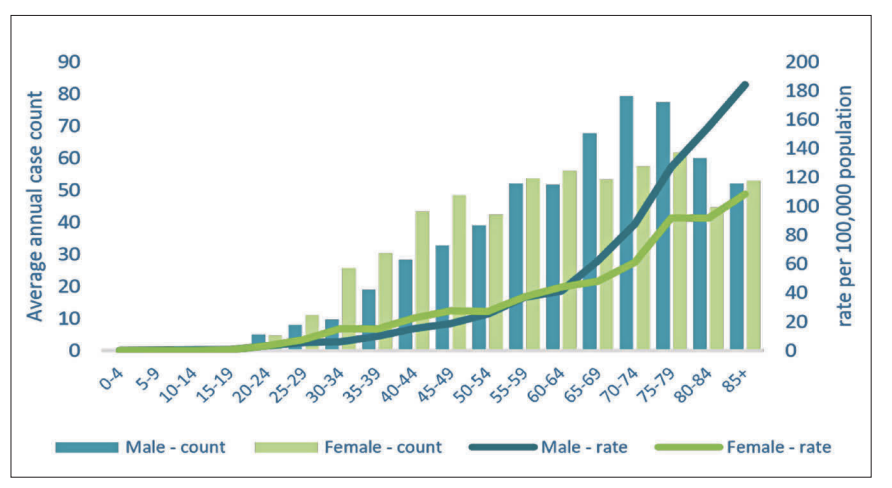
Year-on-year the numbers of melanomas diagnosed in Ireland have increased in both men and women, as per the below graph from the NCRI (Figure 1). The distribution of melanomas diagnosed in Ireland shows higher rates in the southeast and south of the country, which mirrors the situation in the UK.
NEW CASES 2018-2020
FEMALE
MALE
TOTAL
Number of new cases per year C43 melanoma of skin
586
584
1,170
Incidence rate (cases per 100,000 per year)
27.6
32.1
29.4
Cumulative lifetime risk of diagnosis
1 in 39
1 in 37
1 in 38
Percentage of all invasive cancers (excl NMSC)
5.2%
4.5%
4.8%
Ranking among most common invasive cancers (excl NMSC)
4
4
5
Median age at diagnosis (years)
63
68
66
DEATHS 2018-2020
FEMALE
MALE
TOTAL
Number of deaths per year C43 melanoma of skin
56
106
162
Mortality rate (deaths per 100,000 per year)
2.8
6.5
4.4
Cumulative risk of death to age 75 years
1 in 839
1 in 401
1 in 546
Percentage of all invasive cancer deaths (excl NMSC)
1.3%
2.1%
1.7%
Ranking among most common invasive cancer deaths (excl NMSC)
18
14
17
Median age at death (years)
73
73.5
73
TABLE 1: NCRI data on melanoma incidence and deaths in Ireland (2021)
FIGURE 1: NCRI melanoma new case incidence per age group
Risk factors
Fair skin type is a key risk factor for the development of melanoma. The Fitzpatrick skin type scale (Figure 2) is a numerical system for estimating how human skin responds to UV light. It has six categories, from ‘always burns’ to ‘never burns’, and is based on self-reporting and sun exposure.
People with Fitzpatrick skin type I and II are at increased risk of developing melanoma as melanoma is caused by DNA mutations in melanocytes, and patients with less melanin in their skin are less able to protect their nuclear DNA. The Irish Cancer Society has a tool on its website where patients can determine their Fitzpatrick skin type.
Intermittent strong sun exposure and sunburn history, especially in childhood, have been identified as strong risk factors for melanoma. UV exposure in childhood appears to be a strong driver of mutations in the melanocytic system. There is now strong evidence that people who have ever used a sunbed have an increased risk of melanoma and this risk is even higher in people who start using sunbeds before the age of 35 years.
A family history of melanoma also increases the risk. One in every 10 patients diagnosed with melanoma has a family member with a history of the disease.
IVORY
BEIGE
LIGHT BROWN
MEDIUM BROWN
DARK BROWN
VERY DARK BROWN
Characteristics
Pale skin, light or red hair, prone to freckles. Burns very easily and rarely tans.
Characteristics
Fair skin, likely to have light hair, blue or brown eyes. Some have dark hair but still have fair skin. Usually burns but may gradually tan.
Characteristics
Light olive skin with dark hair and brown or green eyes. Burns with long exposure to the sun but generally tans quite easily.
Characteristics
Brown eyes and dark hair. Burns with very lengthy exposures but always tans easily.
Characteristics
Naturally brown skin, brown eyes, and dark hair. Burns only with excessive exposure to the sun. Skin easily darkens further.
Characteristics
Black skin with dark brown eyes and black hair. Burns only with extreme exposure to the sun. Skin very easily darkens further.
Sun protection
At the greatest risk of developing skin cancer. Needs to protect skin, preferably with clothing.
Sun protection
At the greatest risk of developing skin cancer. Needs to protect skin, preferably with clothing.
Sun protection
Should protect themselves in strong sunshine.
Sun protection
Should protect themselves in strong sunshine.
Sun protection
Protect themselves when outdoors in the sun for a long time.
Sun protection
Protect themselves when outdoors in the sun for a long time.
FIGURE 2: Fitzpatrick skin type scale
Diagnosis
The diagnosis of melanoma is primarily a clinical one. Melanoma can arise as a new mole (50%) or a change to an existing mole according to the ABCDE criteria (50%). It must be borne in mind, however, that it is normal to acquire new moles until your late thirties and also that congenital nevi (a nevus that a child is born with or acquired in early childhood) will grow as a child grows. The ABCDE criteria of melanoma is shown below in the below infographic.
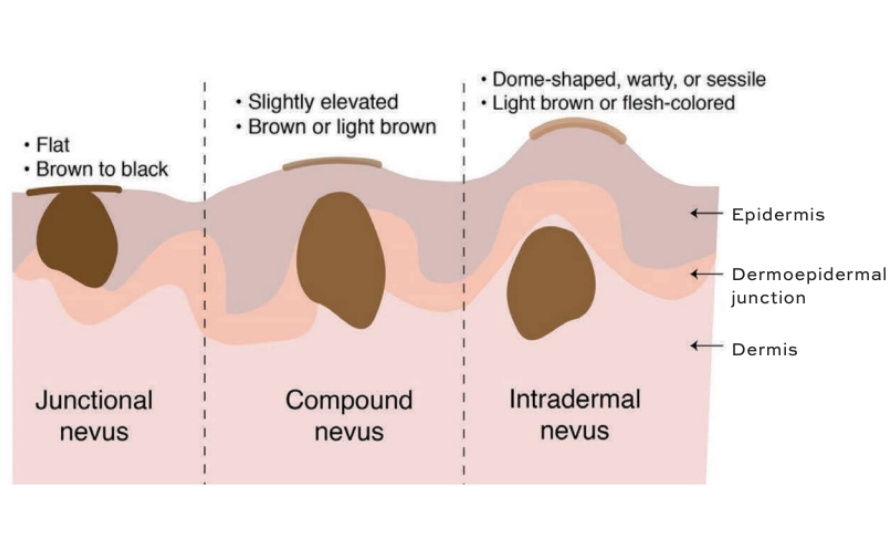
There are three common types of mole or nevi (Figure 3) – junctional nevi, which are flat (and are entirely within the epidermis), compound nevi, which are raised (present in both the epidermis and dermis), and intradermal nevi, which are completely in the dermis.
If an existing mole gets bigger or darker or a new mole arises after 40 years of age, then it is worth referring this patient to a dermatology service. For highly suspicious moles or queried melanomas, patients should be referred to the local pigmented lesion service using the HSE National Cancer Control Programme (NCCP) pigmented lesion referral form.
The patient will then be assessed in the pigmented lesion clinic, with a history of risk factors recorded:
Fitzpatrick skin type;
Recreational sun exposure (number of sun holidays and sunbed use);
Occupational sun exposure (outdoor workers);
Family history of melanoma;
History of blistering sunburn, especially in childhood.
The patient’s moles will then be examined dermascopically and a full or targeted full skin examination carried out. If melanoma is suspected, it is usually excised in the clinic with a cuff of 2mm of tissue-to-fat for histological confirmation.
FIGURE 3: The three types of melanocytic nevi
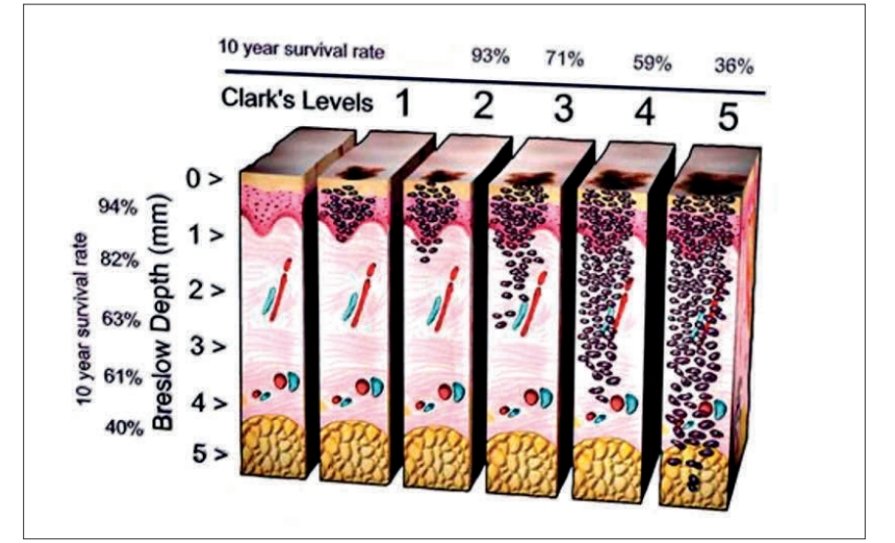
FIGURE 4: Breslow depth scale
Treatment
The primary treatment for early-stage melanoma is surgical excision of the tumour and a margin of surrounding healthy tissue to ensure complete removal. This can be curative in cases where melanoma is localised (stage I and II) and has not metastasised.
The prognosis for melanoma is determined by the thickness (or depth of invasion) of the lesion, known as the Breslow depth (Figure 4).
The Breslow depth also predicates further treatment required and is the tissue denominator in the TNM staging of melanoma (Figure 5).
In patients with melanoma in situ (contained within the epidermis), patients require a wide local excision with a 5mm margin.
In patients with a melanoma up to 0.75mm in depth, a wide local excision with a 1cm margin is required.
In melanoma greater than 0.75 mm in depth, a wide local excision and a sentinel lymph node biopsy is required.
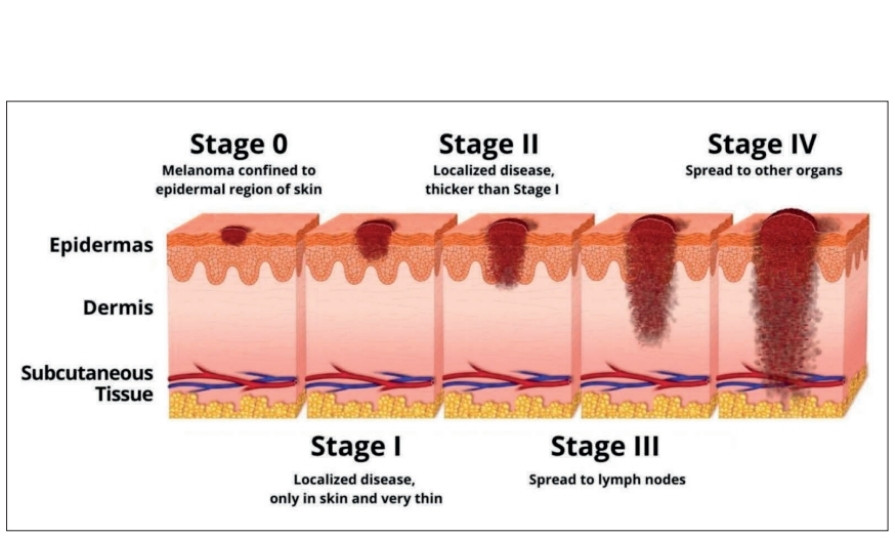
The combination then of Breslow depth, number of draining lymph nodes involved, and whether or not there is evidence of metastases, are used to determine the final clinical staging of melanoma as per the eighth edition of the American Joint Committee on Cancer Staging System (Figure 6).
Follow-up
For patients with melanoma in situ, once wide local excision is complete, these patients are educated about changes to look out for in their moles and do not require follow-up.
For patients with stage 1A melanoma, once wide local excision is complete, these patients are seen two to three times in the dermatology department and advised on how to self-examine and then discharged.
For stage IB to IIIA, patients are seen every three months for three years and then every six months for up to five years. Stage IIIB and IIIC are seen every six months for a further five years for a total of 10 years.
The NCCP has recently published guidelines for the staging and radiological follow-up of melanoma. This guideline was issued in May 2024 and will be considered for review by the NCCP in three years.
Advanced melanoma
The treatment of melanoma has been revolutionised by the development of targeted therapy and immunotherapy, particularly checkpoint inhibitors, and these treatments are currently indicated for the treatment of advanced melanoma.
Targeted therapy is used if mutations in BRAF V600 are identified in advanced melanoma – internationally approximately 30 per cent of melanomas have a BRAF V600 but in Ireland this percentage is lower.
Examples of targeted therapies used for melanoma are:
BRAF inhibitors (vemurafenib);
MEK inhibitors (trametinib and dabrafenib.
TNM MELANOMA STAGING OVERVIEW
STAGE
TUMOUR
NODE
METASTASIS
O
Tis
NO
MO
IA
T1a or T1b
NO
MO
IB
T2a
NO
MO
IIA
T2b or T3a
NO
MO
IIB
T3b or T4a
NO
MO
IIC
T4b
NO
MO
IIIA
T1a/b or T2a
N1a or N2a
MO
IIIB
T0 T1a/b or T2a T2b or T3a
N1b or N1c N1b/c or N2b N1a/b/c of N2a/b
MO
IIIC
T0 T1a/b, T2a/b, or T3a T3b or T4a T4b
N2b/c or N3b/c N2c or N3a/b/c Any N ≥N1 N1a/b/c or N2a/b/c
MO
IIID
T4b
N3a/b/c
MO
IV
Any T, Tis
Any N
M1
N = Number of tumour-involved regional lymph nodes; M = Number of metastases at distant site; T = Primary tumour thickness.
FIGURE 5: TNM staging of melanoma
FIGURE 6: Four stages of melanoma (AJCC)
Immunotherapy unblocks receptors on cytotoxic T-cells which have been blocked by cancer cells and boosts the immune response to melanoma. The two types of immunotherapies most commonly used to treat melanoma are anti-PD-1 drugs and CTLA-4 inhibitors.
Examples of immunotherapies used for melanoma are:
PD1 inhibitors (pembrolizumab and nivolumab);
CTLA-4 inhibitors (ipilimumab).
The majority of regimens include a combination of a targeted agent and immunotherapy.
Several trials are ongoing assessing the use of these treatments in the neoadjuvant setting, ie, prior to surgery. As per European Society for Medical Oncology (ESMO) data, neoadjuvant therapy is the standard of care for resectable stage ≥IIIB melanoma, and considerable benefits have recently been observed with immunotherapy in this setting. In updated findings from two key studies presented at the ESMO Congress 2024 (Barcelona, 13-17 September), long-term survival benefits were reported with various neoadjuvant immunotherapy combinations.
There are also exciting developments in therapeutic anti-cancer vaccines for melanoma and the use of chimeric antigen receptor (CAR) T cell therapy for metastatic melanoma.
Conclusion
Although treatments are evolving for melanoma, and long-term survival has improved significantly in the last decade, even in metastatic disease, thanks to the availability of different treatment options and combination therapies as discussed, it should be recognised that early detection leads to better prognosis and lower treatment burden, with only surgery required. The risk of melanoma can be greatly reduced by being safe in the sun and avoiding the use of sunbeds.
Useful resources for patients: Irish Cancer Society: www.cancer.ie Irish Skin Foundation: www.irishskin.ie
Prof Anne-Marie Tobin PhD FRCPI, Consultant Dermatologist Tallaght University Hospital, Clinical Professor in Dermatology Trinity College Dublin and Clinical Lead in Dermatology Health Service Executive