NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Irish Osteoporosis Society President Prof Moira O’Brien outlines her concerns that Irish patients are being put at risk through failures to adequately monitor potential bone loss and being advised on unsuitable exercise regimens
There is a new trend that has recently started where several DXA clinics are telling patients to come back for repeat DXA scans in five years’ time. I personally find this unacceptable and appalling medical care for our most vulnerable patients.
I have never heard of another disease that causes horrific irreversible skeletal damage where patients are told they are not going to be monitored/reassessed for five years. With cardiac issues etc, the patient will usually develop signs or symptoms that are visible when there is an issue. With bone loss being silent and having no signs or symptoms until a fracture occurs, many will lose their independence, and others will face premature death, which is why this disease is called ‘The Silent Killer’.
People are encouraged to try to prevent and detect early diseases like type 2 diabetes and cancer to name a few, but with bone loss those who are proactive are now being discouraged. It makes absolutely no sense and I personally believe it is playing Russian roulette with people’s lives, especially since research shows that most fractures are preventable. I have patients aged 80-years-old and older who have improved their bone density and reduced their risk of fractures, but I also have 20-year-olds with vertebral fragility fractures.
Most hospitals, due to patient volume, have difficulty accessing initial and repeat DXA scans, which is why our health service should be investing in more DXA scan machines for hospital settings, as prevention of fractures has been proven to be cost effective.
Diagnosis
The diagnosis rate for osteoporosis is only 19 per cent and the highest risk group is women aged over 65, with many of those undiagnosed despite being in and out of the hospital system with fragility fractures and comorbidity risk factors. Considering that many treatments and medications which cause bone loss are given to patients when in hospital, an incentive similar to the very successful hip fracture BPT (Best Practice Tariff) payment should be considered to increase the diagnosis of those at high risk of fracture, and those with undiagnosed vertebral fractures. We are not living in a poor country and no one should end up disfigured with multiple fractures, loss of independence, and premature death when this disease is preventable and treatable in the majority of people.
Causes
Examples of treatments or medications given in hospital settings that cause bone loss include chemotherapy, radiation, aromatase inhibitors, hysterectomies, organ transplants, corticosteroids, and proton pump inhibitors (PPIs) to name just a few.
Patients who are being treated for cancer with radiation, chemotherapy, androgen deprivation treatment, LHRH analogues, testosterone suppression, leuprorelin, or aromatase inhibitors for breast cancer, should all be referred to have a DXA scan. Since all of these treatments are known to cause bone loss, patients need to be treated proactively, not reactively. A bone health action plan should be put in place and their bone health monitored closely.
The Government needs to invest in sports facilities in schools to help not only decrease the risk of bone loss in later life, but also to help decrease diabetes, obesity, depression, heart disease, etc.
About 60 per cent of the bone that a person will have is laid down between the ages of eight to 20 years. The World Health Organisation recommends that all children and adolescents should do at least 60 minutes weight-bearing exercise a day.
A 10 per cent increase of peak bone mass in children is thought to reduce the chance of breaking a bone from osteoporosis in adult life by 50 per cent.
Examples of patients who should be referred for DXA scans while being inpatients
1. A woman aged 40 receiving chemotherapy and/or radiation for ovarian cancer, which is going to put her into early menopause and thus increase her risk for bone loss. While being under the stress of hoping to survive cancer, she should be warned of the secondary effects of her cancer treatment, high stress levels, and the effects of an early menopause, and she should be treated proactively.
If she is not referred for a baseline DXA scan, she may already have unknown low bone mineral density (BMD). Also, if she is not referred for a DXA scan, she could be left in a position of surviving cancer, but losing her independence due to fractures that could have been prevented. If she is not referred for a DXA scan in the near future, this woman will be re-admitted with fractures that could have been prevented.
2. A 60-year-old female, postmenopausal (but was never advised that this would place her at risk for bone loss), on corticosteroids, has rheumatoid arthritis, and has already fractured her radius twice. At some point, this woman will be re-admitted with further fractures that yet again could have been prevented. A DXA referral should be initiated.
3. A 70-year-old male, history of a fractured ankle from tripping but not falling and a radius fracture from pushing himself up from his wheelchair, on PPIs for years, with undiagnosed back pain, postural changes and loss of height having already occurred. A DXA with a lateral vertebral assessment should be done, as he more than likely has thoracic vertebral fractures.
Note: All wheelchair users are high-risk for bone loss, due to the lack of weight-bearing exercise.
A DXA scan exposes a patient to 10 per cent of the radiation of a regular chest x-ray. Similarly, if a person flies from Dublin to New York, they will be exposed to more radiation than when having a DXA scan done.
If bone markers show bone loss is still occurring, a repeat DXA will need to be done to see what area is now at higher risk of fracturing.
Many GPs do not have access to order bone markers which measure how much and how quickly a patient is losing bone and, unfortunately, they are not cheap tests. A DXA scan is cheaper at approximately €120 and also assists with monitoring the specific areas of bone loss.
I have found that compliance is much higher with osteoporosis treatments when a patient can see an improvement on their DXA scan results, and increased compliance is even higher when a patient is shown that their DXA scan results have declined.
Those who can improve their bone health may be able to discontinue the prescribed treatment. Those patients in this category are usually people who do not have a condition or are not on a medication or lifestyle that causes bone loss. Many would have gone through the menopause and lost significant bone secondary to it.
I have also found that those who witnessed/took care of family members who had major osteoporotic fractures are the most proactive regarding wanting to ensure they do not end up like their family members. Since high cortisol levels due to stress can increase bone loss, these type of patients usually become higher risk of fracturing if declined assessment. In one case recently, a man whose T-scores were declining had severe osteoporosis and was told by a consultant to “come back to me when you fracture…”.
A survey in Ireland in 2023 showed the following8
▶ One-in-five adults have fractured a bone since turning 40.
▶ Over one-third were reported to have had a fragility fracture.
▶ The rate of fragility fractures was highest amongst 40-to-54-year-olds.
The fact that some individuals are pushing for only those aged 65 and older to have DXA scans in light of the aforementioned survey results and considering that research also shows that most fractures occur with a DXA result of moderate to marked osteopaenia, which is a T-score between -1.5 to -2.49 is baffling.
▶ The Irish Osteoporosis Society (IOS) recommends annual DXA scans for those who have fractured or are very high risk to fracture (-3.) or higher.
▶ The IOS recommends those who have not fractured but are at risk of fracture should be rescanned every two to three years.
▶ The IOS recommends if a patient’s DXA scan is normal, but they have risk factors for bone loss, they should be monitored at least every three years to prevent fractures occurring.
As it is much cheaper and less painful to prevent fractures than to treat them, especially hip and vertebral due to the horrific irreversible consequences they cause.
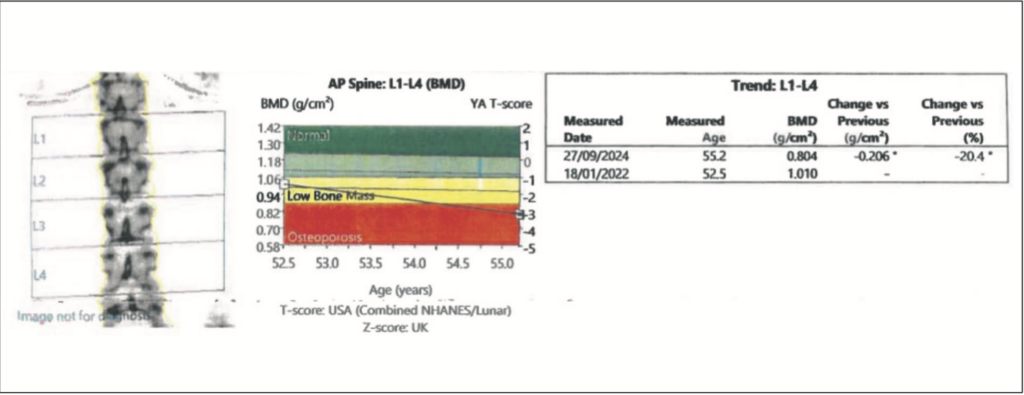
Figure 1 shows an example of a 55-year-old woman who lost 20.4 per cent of bone density in her spine over 20 months due to the menopause. Her non-dominant neck of femur declined by 10.2 per cent, 7 per cent in her total hip, with a 6.6 per cent decline in her dominant hip and 3.2 per cent decline in her dominant total hip.
She was thoroughly investigated and the only risk factor the patient had was that she was post-menopausal. She had no other risk factors for bone loss. These results show why bone loss should be monitored closely.
Denosumab
Dentists should not be telling patients to defer their denosumab injection as they are placing them at risk of spontaneous vertebral fractures. The only person who should be instructing a patient to put their osteoporosis treatment on hold is the prescribing physician.
The IOS, in conjunction with experts in the dental and bone health arena, has put together an information document regarding dental work and denosumab, including issues related to medication-related osteonecrosis of the jaw. For a copy please email info@irishosteoporosis.ie.
Types of exercise not recommended for those with bone loss
The presentation by Ms Ciara Shields (Chartered Physiotherapist and a Clinical Specialist in Musculoskeletal Physiotherapy at IONA Physiotherapy in Drumcondra, Dublin) at the 2024 IOS Annual Medical Conference on exercise for those with vertebral fractures was excellent, as inappropriate exercise is, in my experience and that of the IOS, currently rampant.
Considering I was a Professor of Anatomy at Trinity College Dublin for decades, after teaching anatomy for several decades at the RCSI, I would have no hesitation in saying that I am an expert in anatomy. However, I am seeing more patients who have been told they should do yoga for their bone health, which is unbelievable considering anyone who understands basic anatomy would never recommend yoga for those with or at risk of bone loss. The concept of yoga is wonderful, but it was developed when people did not have the knowledge we now have.
The IOS and I do not recommend yoga or chair yoga for anyone, as many of the stretches contain excessive forward flexion stretches. When a person bends forward at their waist, especially if their legs are straight, it compresses the anterior aspect of the lumbar vertebrae, increasing the risk of fractures. It also places excess stress on the discs in the spine and the sciatic nerve, which can cause radiating pain down a person’s leg.
I have had multiple patients who have fractured in yoga classes and unfortunately the IOS receives many calls from people who have fractured vertebrae doing forward flexion stretches, as well as experiencing disc and sciatic nerve problems, which is why we are putting out our views on yoga/forward flexion.
Another area that is, in my view, placing people at risk of fractures is those who are following the Liftmor high-intensity resistance and impact training exercise programme.
Prof Moira O’Brien
With regard to the Liftmor trial
Watson SL, Weeks BK, Weis LJ, Harding AT, Horan SA, Beck BR. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopaenia and osteoporosis: The LIFTMOR Randomised Controlled Trial. J Bone Miner Res. 2018 Feb;33(2):211-220. doi:10.1002/jbmr.3284
My primary concern with this trial is that they relied on self-reporting for adverse outcomes. It is widely accepted that the majority of vertebral fractures are not diagnosed (estimated to be 70 per cent). Many people feel that they have ‘pulled a muscle’ when in fact they have actually fractured a vertebra.
The only non-biased, scientific method of investigating for adverse outcomes would be if these patients had spinal MRI/CT at intervals throughout the programme to investigate for vertebral fracture. Otherwise, I feel it is misleading to say that there were no adverse outcomes, given the accepted lack of reliability with self-reporting.
I note that this trial was published in 2018 and that the Royal Osteoporosis Society has (like the IOS) not advised this type of exercise programme in any of their publications generated by their expert panel, who regularly review the literature.
We have gone through all the literature and the IOS would not recommend high-intensity resistance exercise to anyone with bone loss. Muscles may be strong, but when they pull on a weak bone, the bone can break.
There should not be a rush to increase bone density; any exercise programme should be slowly and steadily increased so as not to place a person at risk of further fractures. For senior citizens who have never lifted weights, active exercises should be initiated, and slowly progressed to lifting weights. This is to ensure long-term compliance with the programme, as many admit to me that they were in agony (muscle and joint) after being assessed and never continued with the programme.













Leave a Reply
You must be logged in to post a comment.