NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Building a sustainable partnership in global surgery
By
Prof Camilla Carroll
- 25th Mar 2022
Women in Surgery Africa members at the Annual International COSECSA Scientific Meeting, Kampala, Uganda, 2019
RCSI Council Member Prof Camilla Carroll provides an overview of global surgery and the College’s collaboration with the College of Surgeons of East Central and Southern Africa
Lack of access to safe, affordable, and timely surgical care can have a significant negative impact on the patient, their family and the wider community. Access to safe surgical care can save lives and alleviate life-long disabilities. Access to timely surgical care can improve the individual patients’ economic activity and potential and have a beneficial impact on their family and community.
The Republic of Ireland, a high-income country (HIC), has weathered the storm of the Covid-19 pandemic cycle over the past two years and the enormous disruptive impact of the cyberattack on the HSE. The professionalism and resilience of the Irish healthcare workforce ensured that acute patient care was delivered during these challenging times. However, immediate action to address the unacceptably high waiting lists for scheduled care must now be the urgent health priority for 2022. Minister for Health Stephen Donnelly has allocated the biggest ever investment in Ireland’s health and social care services in Budget 2022, with a spend of €21 billion.
A 2022 waiting list action plan of €350 million has been committed by the Minister to stabilise and reduce waiting lists and waiting times for elective surgical care in Ireland, aimed at bringing about significant and lasting change in waiting list numbers.
Currently, it is projected that over 1.5 million patients will be added to active waiting lists in 2022. Minister Donnelly has stated: “While this plan focuses on significant numbers and targets, it is fundamentally about ensuring people receive the right care in the right place, at the right time – reforming our health service through the fundamental principles of Sláintecare.”
The focused spend on scheduled surgical care is on 15 high volume inpatient day case procedures, with the intent that every person waiting for over six months, who is clinically ready, will receive an offer of treatment.
Addressing these treatable surgical diseases in a timely fashion will have a significant impact in reducing the burden of surgical disease experienced by a wide cross-section of Irish patients ranging from the young child requiring tonsillectomy for obstructive sleep apnoea, to the older patient with impaired vision waiting for cataract surgery.
The global burden of treatable surgical disease is staggering. The World Health Assembly, the decision-making body of the World Health Organisation, estimates that treatable surgical disease accounts for 11 per cent of the global burden of disease. Low- and middle-income countries (LMICS) are disproportionately disadvantaged through a lack of access to surgical and anaesthesia care.
Over five billion people lack access to safe, affordable and timely surgical care globally. Over 15,000 children are dying every day because of unmet surgical need in sub-Saharan Africa and southeast Asia.
Women surgeons now represent 14 per cent of COSECSA graduates and 23 per cent of COSECSA trainees
Ireland has acknowledged the need to provide improved and equitable surgical care to the world’s population by developing a strategic collaborative partnership with the College of Surgeons of East Central and Southern Africa (COSECSA). The aim of this collaboration is to “improve the standards of surgical care, education, training, and examinations in the east, central, and southern Africa region”. A memorandum of understating was entered into in 2007 by COSECSA and RCSI, with funding from Irish Aid to help drive forward this partnership. The key individuals who enabled the development of the collaborative programme were the then President of COSECSA Prof Krikor Erzingatsian, a RCSI School of Medicine graduate (class of 1969), and the then President of RCSI Prof Gerry O’Sullivan (2006-2008).
At the time of the signing of the memorandum of understanding in 2007, there were approximately 500 surgeons in the east central sub-Saharan Africa (ECSA) region, serving a population of 230 million. That number has grown to over 1,690 surgeons practising in the region, which represents a figure of 0.53 per 100,000 population. By way of comparison Ireland has a total of 16.74 per 100,000 population practising surgeons.
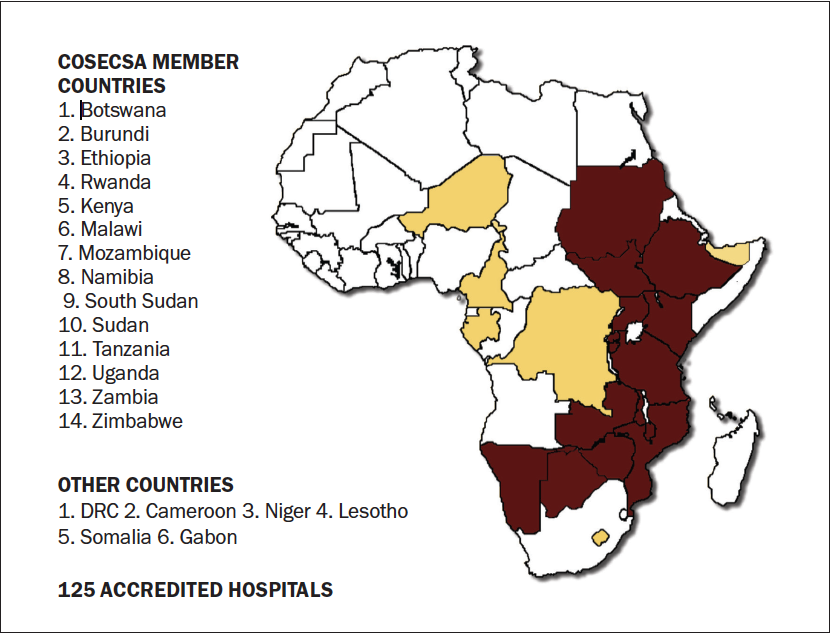
COSECSA is now involved in delivering surgical education and training in over 125 accredited hospital sites. (Figure 1) Each hospital site has a designated programme director, who oversees and delivers a validated surgical curriculum. The surgical trainees utilise an electronic surgical logbook, which has been developed and adapted by COSECSA in partnership with RCSI. This records individual trainee data, including the number and complexity of surgical cases observed and carried out by the surgeon in training.The collection of robust data sets using a validated electronic logbook has been shown to assist in mapping trainee performance and progression. It also acts as a tool to analyse quality of individual training sites.
The surgical training programme involves two years of core surgical training with exposure to general surgery and orthopaedics with a membership examination upon completion of year two. The surgeon in training can then progress to specialised surgical training and exposure to the eight specialties that are currently offered by COSECSA. These include: General surgery; orthopaedics; urology; otolaryngology; cardiothoracic surgery; neurosurgery; plastic and reconstructive surgery; and paediatric surgery. Upon completion of three to four years for specialist training, the surgeon can then undertake the specialty COSECSA Fellowship examination.
A strategic goal of COSECSA to train 500 surgeons by 2020 has been achieved. It is planned to scale-up between 2021- 2025 with 1,000 surgeons to be trained in the coming five years.
Irish Aid has provided over € 5 million to the COSECSA-RCSI collaboration programme, since 2008. Through the collaboration programme, over the past 13 years, 530 surgeons have been trained and graduated with a Fellowship qualification from COSECSA. These Fellows have become part of the specialist surgical workforce in sub-Saharan Africa. This represents a cost of approximately €9,400 per specialist surgeon to the Irish State.
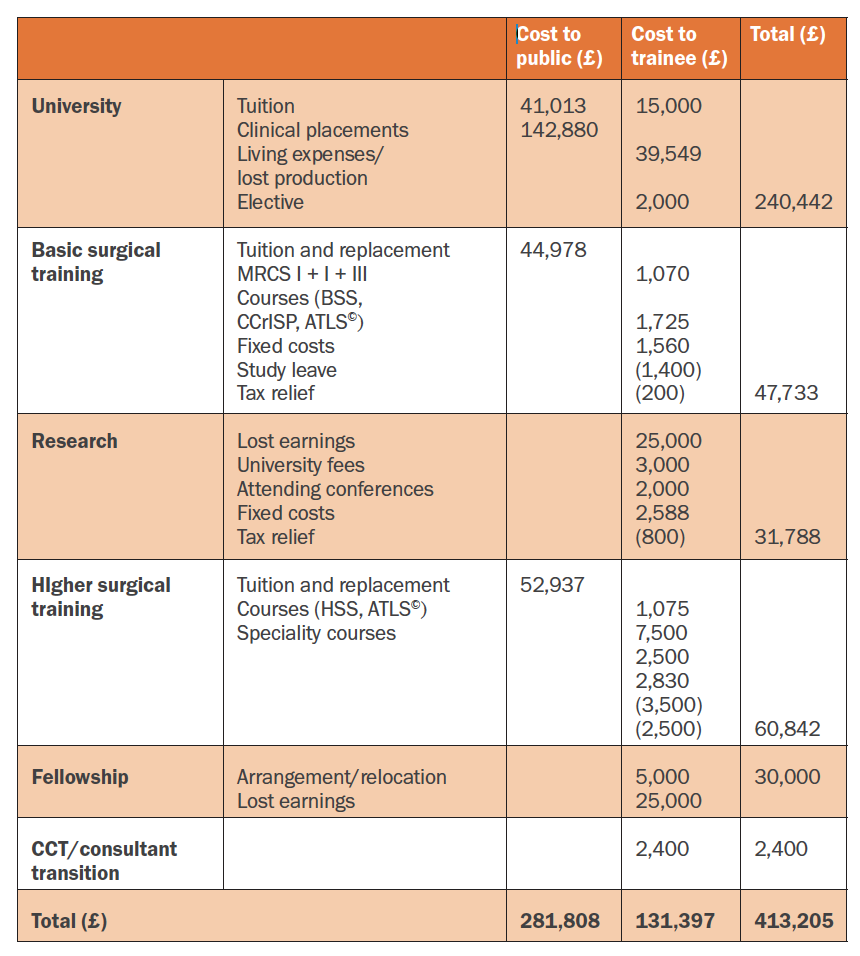
The cost of training a surgeon in Great Britain and Ireland far exceeds this number.
When the RCSI-COSECSA collaboration programme was established in 2007, a position statement from the Association of Surgeons in Training (ASIT) of Great Britain and Ireland outlined the costs of training a surgeon in 2007 to be in the region of £413,205. (Table 1)
Retention
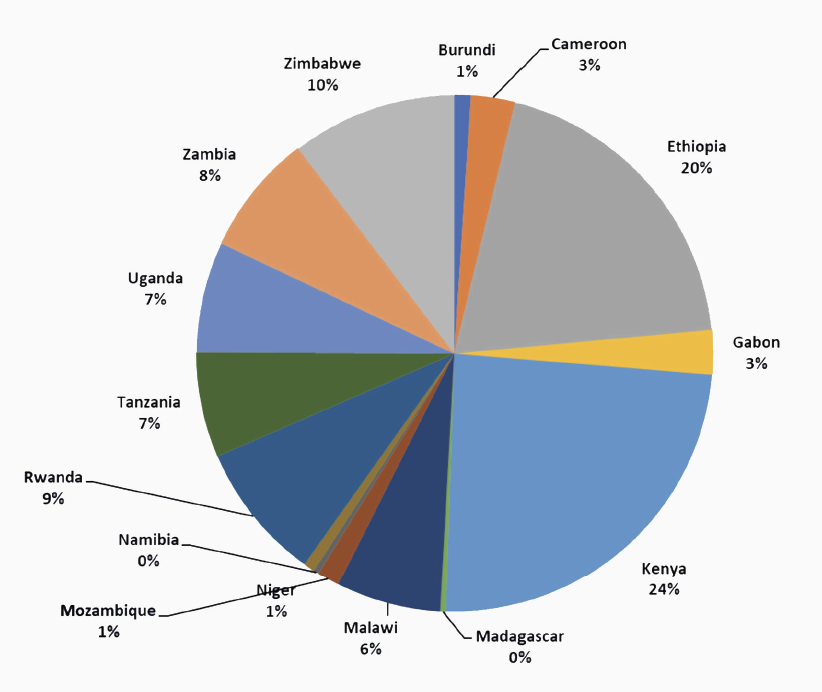
Retention of surgeons in the ECSA region having completed surgical training is 88.13 per cent. The majority of COSECSA trained surgeons were retained within Africa (93.4 per cent). Research carried out at the RCSI by Dr Avril Hutch and published in the World Journal of Surgery in 2017 concluded: “High surgical graduate retention rates across the region indicate that the expansion of national surgical training initiatives is an effective solution to addressing the surgical workforce shortage in East, Central, and Southern Africa and counters long-held arguments regarding brain drain in this region.” (Figure 2)
Figure 1: COSECSA Region. 14 constituent member countries and trains in 20 countries Figure 2: COSECSA graduates by country 2002-2020
This is in stark contrast to the findings of a longitudinal medical career tracking study by the health workforce research group at the RCSI led by Prof Ruairi Brugha. They concluded: “Medical workforce stressors continue to undermine Ireland’s ability to achieve medical workforce sustainability and compliance with the WHO Global Code on international recruitment of health personnel. These include i) high rates of emigration among Irish medical school graduates attracted by working conditions, training, and career opportunities in other English-speaking countries; ii) the need to be compliant with the European Working Time Directive, which restricts hospital doctors working week.”
Global health research has identified the ever-increasing trend that healthcare is being delivered by women. Some 75 per cent of the global health workforce are women, with a representation of over 90 per cent in nursing and midwifery. The recruitment of women into the surgical workforce in the ECSA region has been slow. The RCSI published data in 2016 on the specialist surgeon workforce in the ECSA region and identified that only 9 per cent of the surgical workforce was provided by women surgeons. Women’s under-representation in surgical roles frequently is as a result of societal norms, lack of educational and training pathways, which support women’s careers and visible role models. Motherhood and surgery may not be compatible in societies, where there is no affordable childcare and the burden of domestic work and caregiving is borne by the woman.
Recognising that women were under-represented in the numbers of surgeons being trained in the ECSA region, Women in Surgery Africa (WiSA) was established in 2015. The aim of WiSA is to encourage women to enter surgical training and to support and mentor them during their training. The programme is delivered as a collaborative venture with support from the RCSI and the American College of Surgeons (ACS). The ACS also offer WiSA funded scholarships for training and professional exam fees. WiSA mentoring has had a positive impact on increasing the numbers of women choosing surgery as a career in sub-Saharan Africa. Women surgeons now represent 14 per cent of COSECSA graduates and 23 per cent of COSECSA trainees.
The WHO Global Health 50/50 report seeks to advance action and accountability for gender equality in global health: “Gender equality in health means, that women and men, across the life-course and in all their diversity, have the same conditions and opportunities to realise their full rights and potential to be healthy, contribute to health development, and benefit from the results.” Collaborative trusted partnerships between LMICs and HICs have been the cornerstone of significant advances in global surgery. The COSECSA-RCSI collaboration has been one of the most successful programmes delivering surgical education, training, and assessment, with the end result being an expansion of the surgical workforce in Africa. This success has been enabled by the development of mutual trust between the two organisations, an ethical and culturally sensitive approach to surgical training and education, with institutional leadership locally and nationally. COSECSA is now a well-established surgical training institution offering internationally recognised qualifications. COSECSA works closely with the Colleges of Medicine of South Africa, the west African College of Surgeons, all of the Royal Surgical Colleges in the UK and Australia, the ACS and the Japanese Surgical Society. The strategic plan for COSECSA 2020-2025 is to continue to “scale-up” the number of appropriately trained, well-qualified surgeons and support the development of the anaesthesia, perioperative nursing and obstetrical workforce. A key enabler to surgical workforce expansion is to deliver continuous professional development for the trained surgeons and to this end COSECSA plan to establish a surgical simulation skills centre in Lakilaki Land, Arusha, Tanzania. This exciting project will be the first of its kind in Africa. The location has been carefully selected. Arusha is a multicultural city, a diplomatic hub hosting the UN and the African Court of Human and People’s Rights and home to a number of universities. COSECSA will launch this project and seek donor funding in the coming months.
It is a privilege and honour to collaborate with my friends and surgical colleagues from COSECSA and witness at first hand the impact that building sustainable partnerships in global surgery can have on delivering safe, effective, and affordable surgical care in Africa.
It is important to thank and acknowledge the commitment of Irish Aid on behalf of the people of Ireland in funding this very important work, which has significantly increased the surgical workforce in the ECSA region.
Prof Camilla Carroll, Consultant Otolaryngology Head and Neck Surgeon, Royal Victoria Eye and Ear Hospital, Dublin; Global Surgery Advocate; WiSA Mentor; and RCSI Council Member.










Leave a Reply
You must be logged in to post a comment.