







Dr Mohd Faisal looks at the diagnosis and treatment of refractory depression
Case report
Mr X is a 43-year-old married teacher of two children, who is living with his wife and children. He is happily married for the last 13 years and has a good relationship with his wife. His wife is very supportive towards him. He does not smoke and drinks alcohol occasionally with his friends. He does not take any illicit drugs.
Mr X experienced his first episode of depression at the age of 35 and was initially treated by his GP. His GP prescribed the SSRI sertraline 50mg mane, which was increased to sertraline 100mg mane after a gap of two weeks. Mr X benefited with sertraline and a short course of cognitive behavioural therapy (CBT). However, after six months he relapsed into his depression and as a result he was referred to psychiatric specialist services at the age of 36. So far Mr X has experienced four episodes of depression.
Currently he is presenting with two months history of low mood, loss of enjoyment, poor appetite, lethargy and poor concentration. He is also presenting with middle insomnia and early morning awakening. Collateral history from his wife indicated Mr X has been isolating himself in his bedroom mostly and avoiding meeting his friends for the last two months. His wife described him as being “lost in his own world”. There are no family or financial worries. He is not drinking alcohol. There are no thoughts of self-harm or suicidal ideation/intent or plan. And there is no past history of self-harm.
Mr X is on sick leave from his work for the last four weeks due to his current mental state.
There is no medical history and no family psychiatry history. He consulted with his GP about three months ago and the GP has ruled out any underlying organic causes for his current presentation.
Upon reviewing his clinical notes, it was noticed that Mr X was tried on sertraline 200mg mane with limited improvement in his depressive symptoms. As a result, he was switched from sertraline to the SNRI venlafaxine 75mg mane and later on it was increased to venlafaxine 150mg mane. Although there was some improvement in his mood, his energy level remained low and other symptoms persisted. After waiting for another two weeks, his venlafaxine dose was increased from 150mg mane to 225mg mane. Mr X was followed up regularly in the outpatient clinic for another six weeks and no further improvement in his mood was reported. He continued to experience low mood, anhedonia, poor energy levels, poor concentration and early morning wakening. At this stage, he was given a diagnosis of treatment-resistant depression.
Therefore, an augmentation therapy was considered by the multidisciplinary team. Mr X was started on quetiapine, an atypical antipsychotic used for the treatment of schizophrenia, bipolar disorder, and major depressive disorder, which was gradually increased to 300mg nocte.
In addition, his venlafaxine dose was increased to 300mg mane. He was also started on CBT by the clinical psychologist on the team.
This combination of venlafaxine 300mg mane, quetiapine 300mg nocte and CBT appeared to be very effective for Mr X. There was resolution in his depressive symptoms within two-to-three weeks. He started enjoying things that he used to enjoy in the past. There was a significant improvement in his appetite and he was noted to be sleeping well by his family member. His energy levels and concentration both have improved and he was looking forward to restarting his work.
After six months, his mental state remains stable, however, Mr X has highlighted that he has gained around 5kgs in the last six months and he was advised about healthy diet and exercise.
Depressive disorders are very common with a prevalence of up to 10 per cent in primary care settings, with women being affected twice as likely as men. Depression is ranked as the fourth most common cause of disability worldwide.
Treatment for depression is available, which is highly effective, yet depression is often undiagnosed and undertreated. It should be noted that depression is associated with significant mortality and morbidity. Depression is commonly associated with passive death wishes, fleeting thoughts of self-harm and thoughts of suicide, depending on the severity of depressive episode. And suicide is the second leading cause of death in people between the ages of 20 and 35 years. Often people presenting with depression have comorbid alcohol and substance misuse.
The exact aetiology of depression remains unknown; however, it is likely secondary to several factors including biological, psychological and social factors. It is well established that psychosocial stressors play an important role in the chronicity and recurrence of depressive episode.
There is ongoing stigma and reluctance to seek help for depression. There is also a widespread myth that medications (antidepressants) used to treat depression are addictive in nature, despite the contrary evidence available today. Although antidepressants are not the only treatment option for mild to moderate depressive episodes, when prescribed it is the duty of the doctor to continue to follow-up on the patient and ensure that antidepressants are given at an effective therapeutic dose and for an adequate time frame.
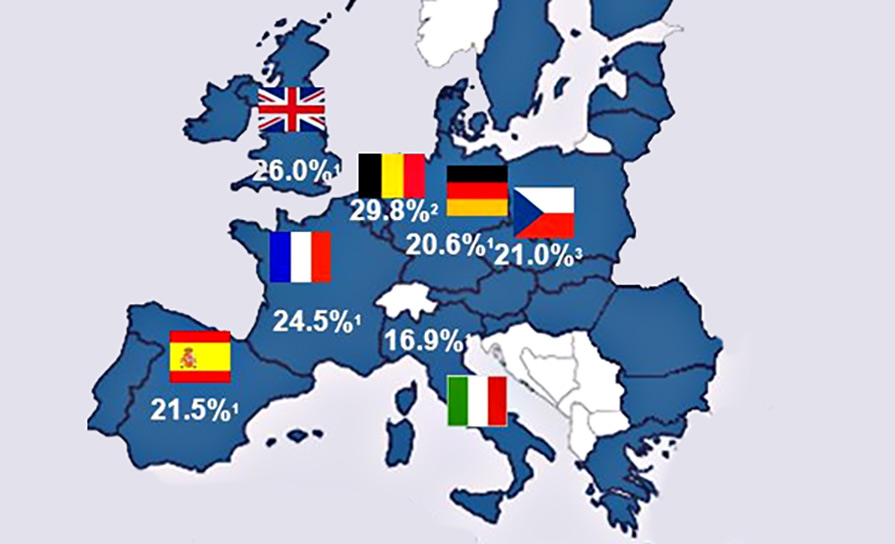
Around one-third of patients presenting with depression do not recover from their depressive symptoms in a timely fashion. This group of patients are classified as having treatment-resistant depression. The exact criteria for treatment-resistant depression remain somewhat controversial. The consensus defines treatment-resistant depression as lack of improvement in depressive symptoms after two adequate trials with two different antidepressants from two different pharmacological classes. In such cases, a diagnostic re-evaluation is essential and once the diagnosis of treatment-resistant depression is confirmed, then a systemic treatment approach should be considered including involvement of multidisciplinary team members in addition to providing pharmacological treatment.
Diagnosis
It is imperative to rule out organic causes of depression. Therefore, blood investigations and a complete physical examination are very important to start with. Hypothyroidism is the most common medical cause which may mimic depression. It is important to keep in mind if a patient is taking an adequate dose of the antidepressant, and they are adherent to the prescribed antidepressant, to rule out Axis II and Axis III disorders and to make sure the patient is not using illicit drugs/alcohol.
At present, treatment-resistant depression is not included in the World Health Organisation’s (WHO) manual of International Classification of Diseases, ICD-10, which is used by psychiatrists in their clinical practice worldwide. However, other different types of depression are listed in the ICD-10. There are specific clinical criteria that should be met for the diagnosis of depression, which is included here from ICD-10.
In typical depressive episodes of all three varieties described below (mild (F32.0), moderate (F32.1), and severe (F32.2 and F32.3)), the individual usually suffers from depressed mood, loss of interest and enjoyment, and reduced energy leading to increased fatiguability and diminished activity. Marked tiredness after only slight effort is common.
Other common symptoms are:
(a) reduced concentration and attention;
(b) reduced self-esteem and self-confidence;
(c) ideas of guilt and unworthiness (even in a mild type of episode);
(d) bleak and pessimistic views of the future;
(e) ideas or acts of self-harm or suicide;
(f) disturbed sleep;
(g) diminished appetite.
There is evidence of persistent low mood which is present most of the day and nearly every day with little variation and lacks responsiveness to changes in the circumstances. Sometimes, people experience worse mood in the morning and the mood improves as the day goes on, which is known as diurnal mood variation. For depressive episodes of all three grades of severity, a duration of at least two weeks is usually required for diagnosis, but shorter periods may be reasonable if symptoms are unusually severe and of rapid onset.
The following are the subtypes of depression obtained from ICD-10:
F32 Depressive episode.
F32.0 Mild depressive episode
00 Without somatic syndrome.
.01 With somatic syndrome.
F32.1 Moderate depressive episode.
.10 Without somatic syndrome.
.11 With somatic syndrome.
F32.2 Severe depressive episode without psychotic symptoms.
F32.3 Severe depressive episode with psychotic symptoms.
F32.8 Other depressive episodes.
F32.9 Depressive episode, unspecified.
F33 Recurrent depressive disorder.
F33.0 Recurrent depressive disorder, current episode mild.
.00 Without somatic syndrome.
.01 With somatic syndrome.
F33.1 Recurrent depressive disorder, current episode moderate.
.10 Without somatic syndrome.
.11 With somatic syndrome.
F33.2 Recurrent depressive disorder, current episode severe without psychotic symptoms.
F33.3 Recurrent depressive disorder, current episode severe with psychotic symptoms.
F33.4 Recurrent depressive disorder, currently in remission.
F33.8 Other recurrent depressive disorders.
F33.9 Recurrent depressive disorder, unspecified.
Management
Once a diagnosis of treatment-resistant depression has been confirmed, it is vital to follow a step-wise approach for the management plan and to involve all the members of the multidisciplinary team.
Augmentation of antidepressants with lithium, antipsychotics, triiodothyronine (a thyroid hormone), lamotrigine (anti-convulsant), use of high-dose venlafaxine (recommended by NICE guidelines), and electroconvulsive therapy (ECT) are well supported in the literature and could be considered.
There is a good evidence for combining olanzapine with fluoxetine. Also, adding quetiapine, aripiprazole or risperidone to the existing antidepressant has been found to be effective. Like any other treatment, some people may experience side effects, such as weight gain, sedation, dry mouth, and restlessness. Therefore, screening for potential side effects is important.
Also, it is important to keep in mind the available psychological interventions like CBT, group therapy and family therapy.
ECT is usually opted as a last-line treatment option for treatment-resistant depression, however, it is an effective, well-established treatment and is wellsupported in the literature in the management of this condition.
References
1. Oxford handbook of Psychiatry, 3rd Edition
2. The Maudsley Prescribing Guidelines in Psychiatry, 13th Edition









Leave a Reply
You must be logged in to post a comment.