







ACE inhibitors and angiotensin receptor blockers are some of the most-used drugs in clinical practice and they have come into increased focus regarding safety of use during the current Covid-19 crisis. Dr Sam Kant explores the origins of this debate and future directions
Uncertain times can spawn many theories, often unfounded. As we face an unprecedented crisis with coronavirus disease 2019 (Covid-19), efforts to mitigate and treat the illness have generated much debate.
One of the foremost discussions is the safety of angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARB) in patients afflicted with Covid-19.
We look to explore reasons why this debate has ensued, current data available from animal and human models, and recommendations for practitioners.
Generation of the hypothesis
The coronavirus gains entry into a host cell via the ACE2 receptor. The ACE2 is abundantly present in the epithelia of the lung and small intestine, which may provide possible avenues for entry of the virus.1 Additionally, the current strain of coronavirus seems to have at least 10-to-20 times higher affinity for the ACE2 in comparison to previous coronavirus strains.2
There is growing concern that ACEi and ARBs can increase the expression of ACE2 and augment viral host entry.
Previous animal studies have shown that ACE2 activity is upregulated by the use of ACEi and ARBs.3,4 This finding, however, has not been replicated in other animal models.5 The same conflict exists in human studies:
1. There is data demonstrating no impact of ACEi/ARBs on ACE2 levels.6,7
2. The debate is further split with respect to ACEi versus ARBs: One study showed olmesartan (an ARB) increased urinary ACE levels in comparison to other ACEi and ARBs,8 while another study showed that ACEi and not ARBs increased ACE2 gene expression.9
This conflicting information still does not help us in deciding whether we should continue ACEi or ARBs in patients who contract Covid-19.
Since the axis of renin, ACE and angiotensin is extremely dynamic, the next step is to examine studies that have looked at use of ACEi/ARBs in the setting of viral stressors.
Use of drugs during viral illness
Animal studies have elucidated that increased ACE2 levels may attenuate viral-induced lung injury in H7N9 influenza infected mouse models.10 Further, a study that examined the crucial role of ACE2 in viral host entry during the coronavirus-associated severe acute respiratory syndrome (SARS) outbreak of 2003 found that blocking the angiotensin I receptor with an ARB improved lung function. Moreover, a study of over 1,000 patients completed at a tertiary care centre in central Texas, US, showed that continued use of ACEi during viral pneumonia was associated with improved outcomes.11
However, patients who continued ACEi in that study did not have as severe disease as those in whom it was discontinued.
There is preliminary data now available from China involving Covid-19 patients, which makes the case that use of ACEi and ARBs might be protective and that patients on these medications may have less-severe disease.12,13
However, these studies cannot be deemed conclusive, given these are retrospective analyses, have low sample size and have inadequately adjusted statistics.
From here on now
Given that there is a lack of robust evidence to guide the use of these agents in the setting of Covid-19-infected patients, we currently have to rely on consensus from expert guidelines.
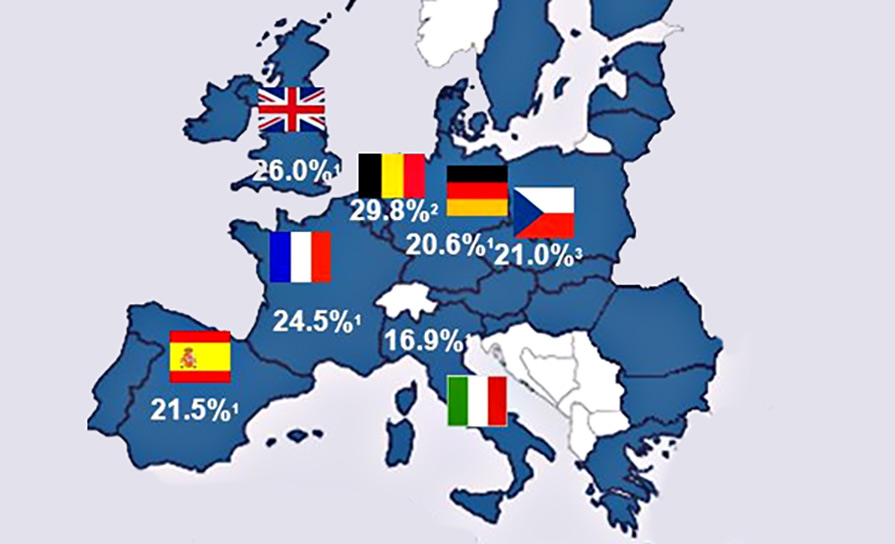
Various societies have sought to quell this uncertainty by releasing statements, such as the following from the Council on Hypertension of the European Society of Cardiology (at the time of writing): “The Council on Hypertension strongly recommends that physicians and patients should continue treatment with their usual anti-hypertensive therapy because there is no clinical or scientific evidence to suggest that treatment with ACEi or ARBs should be discontinued because of the Covid-19 infection”.14
Many other societies in Europe have followed similar directives, such as the European Renal Association, European Society of Hypertension, UK Renal Association and Spanish Society of Hypertension.
This debate has not only prompted the research community to look for answers to this pertinent question, but has also opened avenues for exploring much-needed therapeutics against this daunting disease.
References
1. Hamming V, Timens W, Bulthuis M, Lely AT, Navis GJ, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. Journal of Pathology. 2004;203(2):631-637. https://www.narcis.nl/publication/RecordID/oai:pure.rug.nl:publications%2F1ca9e614-055e-4acf-b2e6-2cde1c491e8b. doi: 10.1002/path.1570.
2. Wrapp D, Wang N, Corbett KS, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science (New York, NY). 2020;367(6483):1260-1263. https://www.ncbi.nlm.nih.gov/pubmed/32075877. doi: 10.1126/science.abb2507.
3. Batlle D, Ye M, William J, Wysocki J, Soler MJ, Lloveras J. Localisation of ACE2 in the renal vasculature: Amplification by angiotensin II type 1 receptor blockade using telmisartan.(angiotensin-converting enzyme) (author abstract). The American Journal of Physiology. 2009;296(2):F398.
4. Ferrario CM, Jessup J, Chappell MC, et al. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation. 2005;111(20):2605-2610. http://circ.ahajournals.org/cgi/content/abstract/111/20/2605. doi: 10.1161/CIRCULATIONAHA.104.510461.
5. Burchill LJ, Velkoska E, Dean RG, Griggs K, Patel SK, Burrell LM. Combination renin–angiotensin system blockade and angiotensin-converting enzyme 2 in experimental myocardial infarction: Implications for future therapeutic directions. Clinical Science (London, England: 1979). 2012;123(11):649-658. https://www.ncbi.nlm.nih.gov/pubmed/22715807. doi: 10.1042/CS20120162.
6. Burrell LM, Risvanis J, Kubota E, et al. Myocardial infarction increases ACE2 expression in rat and humans. European Heart Journal. 2005;26(4):369-375. https://www.ncbi.nlm.nih.gov/pubmed/15671045. doi: 10.1093/eurheartj/ehi114.
7. Ramchand J, Patel SK, Srivastava PM, Farouque O, Burrell LM. Elevated plasma angiotensin converting enzyme 2 activity is an independent predictor of major adverse cardiac events in patients with obstructive coronary artery disease. PloS One. 2018;13(6):e0198144. https://www.ncbi.nlm.nih.gov/pubmed/29897923. doi: 10.1371/journal.pone.0198144.
8. Furuhashi M, Moniwa N, Mita T, et al. Urinary angiotensin-converting enzyme 2 in hypertensive patients may be increased by olmesartan, an angiotensin II receptor blocker. AJHYPE. 2015;28(1):15-21. https://www.ncbi.nlm.nih.gov/pubmed/24842388. doi: 10.1093/ajh/hpu086.
9. Vuille-dit-Bille RN, Camargo SM, Emmenegger L, et al. Human intestine luminal ACE2 and amino acid transporter expression increased by ACE-inhibitors. Amino Acids. 2015;47(4):693-705. https://www.ncbi.nlm.nih.gov/pubmed/25534429. doi: 10.1007/s00726-014-1889-6.
10. Yang P, Gu H, Zhao Z, et al. Angiotensin-converting enzyme 2 (ACE2) mediates influenza H7N9 virus-induced acute lung injury. Scientific Reports. 2014;4(1):7027. https://www.ncbi.nlm.nih.gov/pubmed/25391767. doi: 10.1038/srep07027.
11. Henry C, Zaizafoun M, Stock E, Ghamande S, Arroliga AC, White HD. Impact of angiotensin-converting enzyme inhibitors and statins on viral pneumonia. Baylor University Medical Center Proceedings. 2018;31(4):419-423. http://www.tandfonline.com/doi/abs/10.1080/08998280.2018.1499293. doi: 10.1080/08998280.2018.1499293.
12. Yingxia Liu, Fengming Huang, Jun Xu, Penghui Yang, Yuhao Qin, Mengli Cao, Zhaoqin Wang, Xiaohe Li, Shaogeng Zhang, Lu Ye, Jingjun Lv, Jie Wei, Tuxiu Xie, Hong Gao, Kai-Feng Xu, Fusheng Wang, Lei Liu, Chengyu Jiang. Anti-hypertensive angiotensin II receptor blockers associated to mitigation of disease severity in elderly COVID-19 patients. Preprint MedRxiv.
13. Guang Yang, Zihu Tan, Ling Zhou, Min Yang, Lang Peng, Jinjin Liu, Jingling Cai, Ru Yang, Junyan Han, Yafei Huang, Shaobin He. Angiotensin II receptor blockers and angiotensin-converting enzyme inhibitors usage is associated with improved inflammatory status and clinical outcomes in Covid-19 patients with hypertension. MedRxiv.
14. European Society of Cardiology. Position statement of the ESC council on hypertension on ACE-inhibitors and angiotensin receptor blockers. Published march 13, 2020. https://www.escardio.org/Councils/Council-on-Hypertension-(CHT)/News/position-statement-of-the-esc-council-on-hypertension-on-ace-inhibitors-and-ang.










Leave a Reply
You must be logged in to post a comment.