NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Cardiac CT evaluates the cause of chest pain and shortness of breath, can check the heart arteries for narrowing or blockages, and can assess the heart valves
Chest pain is a leading cause of referrals both to the emergency department and to cardiology outpatient clinics. Determining a patient’s risk of cardiovascular disease (CVD) is important to avoid the potential morbidity and mortality associated with coronary events. In general practice, a patient’s risk is mostly assessed using validated risk scores like the SCORE2 and QRISK3 scores, which take into account demographic data as well as traditional risk factors including smoking, diabetes, hypertension, and hyperlipidaemia. While it is easy to manage patients at the extreme ends of the spectrum at low- and high-risk, the challenge remains with patients classed as intermediate-risk. Cardiac CT is an excellent tool in the evaluation of patients with and without chest pain, which adds anatomic information to traditional risk scores and guide further investigation and management. The two most commonly-used types of cardiac CT are coronary artery calcium (CAC) score and CT coronary angiography (CTCA). This article will focus on the value of these tests using two illustrative cases.
CAC: What is it?
CAC is a non-contrast CT scan used predominantly in the evaluation of asymptomatic patients, which can successfully re-classify patients as low-risk when used in addition to clinical risk scores.1 It is used to identify the presence and quantify the amount of calcified coronary atherosclerotic plaque. The images are ECG-gated, meaning that image acquisition is timed for a pre-determined phase in the cardiac cycle to limit cardiac motion and resulting in high-quality diagnostic images. As the entire heart cannot be imaged in one cardiac cycle, the images are acquired over three-to-four heartbeats with the table moving the patient between images. The scan takes approximately four seconds during a single breath hold and is well tolerated by patients.
Why use CAC?
There are many advantages to CAC scoring. Firstly, it does not require an IV or IV contrast and avoids the attendant risk of complications. Unlike CTCA, no pre-medication or specific preparation is required. The dose of radiation is low at approximately one millisievert (mSV), which is substantially less than the ~10mSV associated with invasive coronary angiography (ICA).
Who is CAC most suitable for?
CAC should generally be reserved for asymptomatic patients with no known CVD to improve cardiovascular risk prediction. In patients at intermediate- or high-risk who are reluctant to take medications, a CAC can provide concrete evidence of their atherosclerotic plaque burden to enhance their understanding of their disease and re-emphasise the need for preventive medications. In a patient like in Case Report 1, who is seeking further evaluation, this is a safe, non-invasive test with the potential to provide reassurance.
CAC is less useful in younger patients <40 years who are more likely to have non-calcified plaque, which cannot be identified without the use of IV contrast and in whom a negative calcium score may be falsely reassuring.2 CAC also cannot assess the severity of stenosis; therefore, patients with cardiac sounding chest pain should have a more definitive evaluation with a CTCA.
How are the results interpreted?
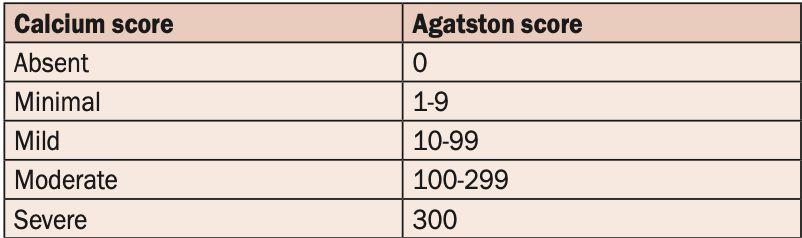
CAC score is presented using the Agatston unit, a validated scoring system for CAC using 3mm CT slices. The results are presented as a number which can then be graded from absent to severe (see Table 1). The score is also converted to a percentile based on the patient’s age, gender, and ethnicity to see how they compare to their peers. A normal CAC score or CAC score of zero is an excellent prognostic indicator with low-risk of CVD out to 12 years of follow-up in one large study.3 Overall, plaque burden as assessed by CAC has been shown to be more predictive of events than degree of stenosis identified on CTCA, highlighting the value of this non-contrast study.4
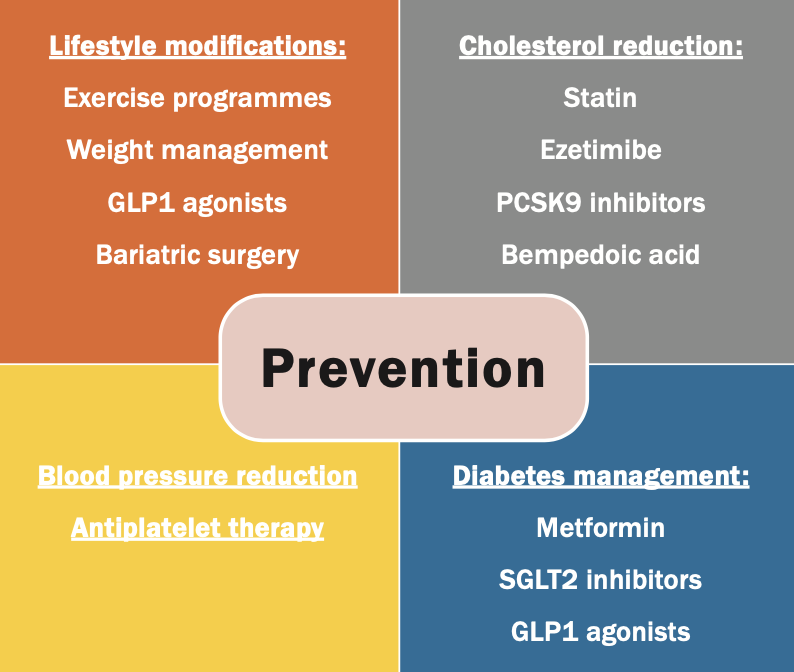
Patients with moderate or severe calcification (CAC >100) should be treated using our full armoury of preventive medications (see Figure 1). Although they may not have had an overt clinical event, this score shows they have demonstrable atherosclerotic disease and are at a higher risk of future events and should therefore be treated more like secondary prevention patients. The use of aspirin in these patients is the subject of debate. One large study demonstrated potential benefit with the use of aspirin in patients with a CAC >100, particularly in those with a Framingham risk score >10 per cent, and therefore aspirin therapy could be discussed with the patient in a shared decision-making capacity.5
Should you repeat a CAC?
The amount of coronary calcium cannot be reduced with therapy and this score should mostly be seen as a ‘one and done’ to evaluate risk. Statins work by stabilising high-risk plaque and reducing the risk of acute rupture, often by increasing vascular calcification, therefore, there is little value in using this test to monitor response to treatment. In patients with a CAC of zero, a warranty period applies of between three-to-seven years, with shorter periods associated with diabetic patients.6 For higher-risk patients with a previously normal CAC score, a repeat scan can be considered.
Case report 1
A 66-year-old asymptomatic female presents for routine review and cardiovascular risk assessment. She is active and walks at least 30 minutes at a brisk pace daily. Her cardiovascular risk factors include hypertension on amlodipine 10mg OD, hyperlipidaemia not currently on statin therapy due to previous side-effects, an ex-smoking history of 30 pack years, and a positive family history with her father dying of a myocardial infarction aged 53 years. She was also started on aspirin for primary prevention many years ago due to her concern regarding her cardiovascular risk and has tolerated this well. She has a normal ECG. Her QRISK3 score is 14.8 per cent, classifying her as intermediate-risk. She would like further definitive evaluation given her family history and has read about CAC score as a potential test.
TABLE 1: Calcium score classification and corresponding Agatston valueFIGURE 1: Currently available cardiovascular prevention therapies. Abbreviations: GLP1: Glucagon-like peptide 1, PCSK9: Proprotein convertase subtilisin/kexin type 9, SGLT2: Sodium-glucose co- transporter 2
Case 1: Results
The patient attended for her test and the result was a CAC score of zero. This is at the lowest percentile for her age, gender, and race. This re-classifies her from intermediate-risk to very low-risk. Her aspirin was stopped due to a greater risk of harm from bleeding than potential benefit from a primary prevention perspective. She was advised to continue her anti-hypertensive treatment to reduce her risk of other vascular events. She was highly reassured by the results and does not feel further investigation is necessary.
Case report 2
A 58-year-old male was referred to cardiology outpatients with two previous episodes of chest discomfort while hill walking. He is asymptomatic within his normal range of physical activity, which includes a 30-minute walk daily. Cardiovascular risk factors include hypertension and hyperlipidaemia on amlodipine 10mg, hydrochlorothiazide 25mg, and atorvastatin 20mg. He has a positive family history with a brother undergoing percutaneous coronary intervention (PCI) aged 54. He is a lifelong non-smoker. His BMI is mildly elevated at 27kg/m2. His systolic blood pressure on treatment is 140mmHg. His QRISK3 score is 14.2 per cent, placing him in the intermediate-risk category. As a patient who has been symptomatic, but is clinically stable, a CTCA could be an appropriate test for him.
Case 2: Results
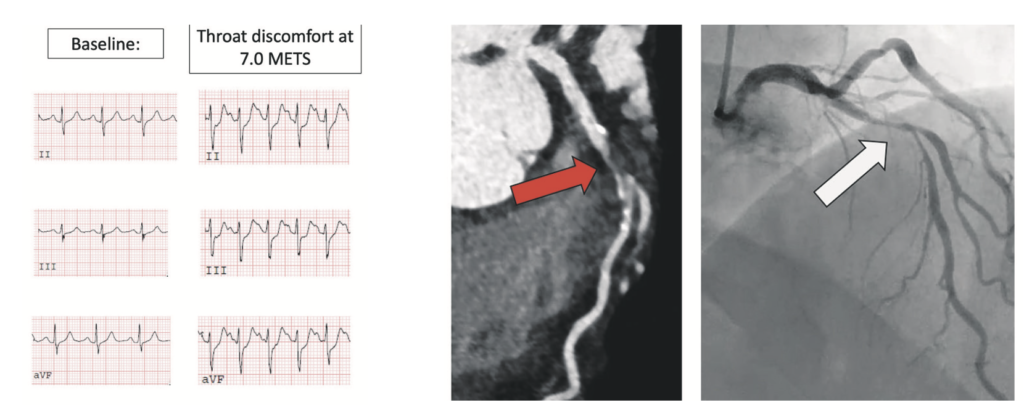
The patient was initially referred for ETT. This was submaximal and stopped as he developed chest and throat discomfort at 7.0 METS, having not achieved 85 per cent of his age-predicted maximal heart rate. There was upsloping ST depression in the inferior leads, which are non-diagnostic ECG changes. He was keen to avoid ICA and so was referred for CTCA. This showed a large amount of mostly non-calcified plaque in the proximal left anterior descending (LAD) artery, extending into the mid LAD and resulting in severe stenosis (70-to-99 per cent) proximal to the origin of the first diagonal vessel. ICA was then performed, confirming severe stenosis of the proximal and mid LAD, and the patient underwent successful PCI to the LAD (see Figure 2). In this case, the CTCA identified the cause of his symptoms in a prognostically-significant location in the LAD.
How is CTCA different from CAC?
CTCA is a form of contrast enhanced ECG-gated study. As well as identifying the presence and amount of calcified plaque, it can also detect non-calcified plaque burden. In addition to this, it can estimate the severity of luminal stenosis resulting from this atherosclerotic plaque. Thinner slices are reconstructed measuring 0.75mm, allowing accurate assessment of the coronaries.
CTCA requires special patient preparation for the test. It requires a large bore (18G) IV cannula to allow for rapid injection of contrast. Heart rate control is more important and a heart rate of less than 60bpm is optimal to achieve diagnostic imaging. To achieve this, patients are given short-acting beta-blockers on the morning of the study. Sublingual nitroglycerin is administered on the table to vasodilate the coronaries and avoid over-estimating the severity of stenosis. The scan itself lasts approximately six seconds, but the preparation can take longer.
Why use CTCA?
In the evaluation of coronary artery disease (CAD), the debate between functional or stress testing versus anatomic testing has been ongoing for years. The exercise treadmill test (ETT) has been the basic workhorse in cardiology, but carries has a low sensitivity of approximately 66 per cent when compared to CTCA ~98 per cent.7 Most patients who can exercise without typical angina will have a normal stress test.8 A normal ETT can also be falsely reassuring, as most events will occur in patients with a previous normal functional study, whereas most events occur in patients with a non-zero calcium score, speaking to the excellent negative predictive value of CTCA compared to ETT.9
The SCOT-HEART trial showed that CTCA improved cardiovascular outcomes (non-fatal myocardial infarction and cardiovascular death) when compared to standard of care.10 This was shown to be related to the increased rates of prescribing of antiplatelet and statin therapies in the CTCA arm compared to the standard of care group, demonstrating the effectiveness of our current preventive therapies.11
Our alternative to ETT has been invasive coronary angiography (ICA), considered to be the gold standard for diagnosing CAD. Although ICA tells us about obstructive stenosis, it cannot give an assessment of overall plaque burden. Furthermore, up to 60 per cent of ICAs are normal in the evaluation of patients with chest pain,12 exposing them to potential risk of complications without any additional benefit over CTCA.
TABLE 2: Results of CT coronary angiogram usually include a description of the type of plaque as well as the severity of stenosis by percentage and graded classification
What patients is CTCA less useful for?
Although CTCA is an excellent test, it is not suitable for all patients. As with any CT requiring IV contrast, patients with severe renal dysfunction CKD IV-V are contraindicated, unless a plan for dialysis is made for after. A prior severe contrast allergy is treated as an absolute contraindication, although patients with a mild reaction, eg, rash, can be pre-treated with steroids and chlorphenamine and proceed safely.
The other relative contraindications relate to patients in whom achieving diagnostic quality imaging may not be possible. The joint AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Chest Pain Guidelines suggested an age cut-off of <65 years for those proceeding to CTCA.13 This was based on results from the PROMISE trial, which found that CTCA was a better prognostic indicator for people under 65 years.14 In patients with atrial fibrillation, the irregular heart rate makes it difficult to ECG-gate the images, which can lead to motion artifacts. Patients with morbid obesity with a BMI of >40kg/m2 will have more image noise, interfering with interpretation. Patients with known CAD and small stents will have extensive calcification resulting in blooming artifacts, limiting the assessment of stenosis in those areas. If patients cannot lie still and perform a breath hold, there may be significant artifacts limiting interpretation. These are all relative contraindications and therefore can be assessed on a patient-by-patient basis.
How are the results interpreted?
In some centres, a non-contrast scan is performed first prior to CTCA and a CAC score will be written in the report. The CTCA results will be presented with each vessel described individually, with a description of the amount and type of plaque in each segment of the vessel, as well as an estimate of severity of stenosis (see Table 2). The presence of coronary anomalies will also be described.
As CTCA identifies any plaque or stenosis, a normal CTCA is reassuring; with excellent negative predictive value, with annual event rates as low as 0.2 per cent in patients with no coronary plaque or stenosis on CTCA.15 The chest pain guidelines suggest a warranty period of approximately two years in those presenting with chest pain with a previously normal CTCA.13
When do we need another test?
In patients who are symptomatic who have a moderate (50-to-69 per cent) or severe (70-to-99 per cent) stenosis on CTCA, further testing can be considered. In the case of a moderate stenosis, the significance of the lesion can be tested with stress testing using either ETT, dobutamine stress echo, or stress MR perfusion. In those with a severe stenosis, the location of the disease can dictate the management. We know from the ischaemia-EXTEND trial that there is no difference in mortality at seven years of follow-up between an early invasive strategy compared to conservative strategy, provided high-risk left main disease was first ruled out by CTCA. The benefit was demonstrated in symptomatic patients with relief of angina.16 This supports the fact that medical management can be instituted safely for more distal disease, provided symptoms can be controlled with medications. ICA is recommended if there is high-risk disease: Left main (>50 per cent stenosis) or three vessel CAD (>70 per cent stenosis) or in the case where the severity of stenosis cannot be assessed due to severe calcification.
CT-fractional flow reserve (CT-FFR) is a non-invasive haemodynamic evaluation of intermediate lesions currently under investigation in patients with stable chest pain that may be useful in the future and avoid the need for ICA.17
Who should refer for cardiac CT?
As with any diagnostic test, the person referring for the test should be confident in how to interpret the results, and in some cases this will require a referral to a cardiology outpatient clinic. Cardiac CT services vary substantially between regions and hospital systems and, in some cases, direct-access GP referral pathways are available. As part of the Sláintecare programme, integrated care cardiology services are increasingly available in the community and a collaborative approach between cardiology and GPs can be used to enhance patient risk stratification and management through the use of cardiac CT.
Conclusion
Cardiac CT is a safe, effective, non-invasive evaluation of patients with and without chest pain to determine cardiovascular risk. It can be used to identify the patients at the highest level of cardiovascular risk who will benefit from the full extent of our preventive therapies, and also identify those who are at very low-risk of future events. CTCA assesses overall plaque burden of both calcified and non-calcified atherosclerotic plaque and can also assess the severity of stenosis so can be used for symptomatic patients and potentially avoid the need for ICA.
References
Winther S, Schmidt SE, Mayrhofer T, Bøtker HE, Hoffmann U, Douglas PS, et al. Incorporating coronary calcification into pre-test assessment of the likelihood of coronary artery disease. J Am Coll Cardiol. 2020;76(21):2421-32
Mortensen MB, Gaur S, Frimmer A, Bøtker HE, Sørensen HT, Kragholm KH, et al. Association of age with the diagnostic value of coronary artery calcium score for ruling out coronary stenosis in symptomatic patients. JAMA Cardiol. 2022;7(1):36-44
Blaha MJ, Cainzos-Achirica M, Dardari Z, Blankstein R, Shaw LJ, Rozanski A, et al. All-cause and cause-specific mortality in individuals with zero and minimal coronary artery calcium: A long-term, competing risk analysis in the coronary artery calcium consortium. Atherosclerosis. 2020;294:72-9
Mortensen MB, Dzaye O, Steffensen FH, Bøtker HE, Jensen JM, Sand NPR, et al. Impact of plaque burden versus stenosis on ischemic events in patients with coronary atherosclerosis. J Am Coll Cardiol. 2020;76(24):2803-13
Miedema MD, Duprez DA, Misialek JR, Blaha MJ, Nasir K, Silverman MG, et al. Use of coronary artery calcium testing to guide aspirin utilisation for primary prevention: Estimates from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Qual Outcomes. 2014;7(3):453-60
Dzaye O, Dardari ZA, Cainzos-Achirica M, Blankstein R, Agatston AS, Duebgen M, et al. Warranty period of a calcium score of zero: Comprehensive analysis from MESA. JACC Cardiovasc Imaging. 2021;14(5):990-1002
Yin X, Wang J, Zheng W, Ma J, Hao P, Chen Y. Diagnostic performance of coronary computed tomography angiography versus exercise electrocardiography for coronary artery disease: A systematic review and meta-analysis. J Thorac Dis. 2016;8(7):1688-96
Rozanski A, Gransar H, Hayes SW, Min J, Friedman JD, Thomson LE, et al. Temporal trends in the frequency of inducible myocardial ischaemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol. 2013;61(10):1054-65
Budoff MJ, Mayrhofer T, Ferencik M, Bittner D, Lee KL, Lu MT, et al. Prognostic value of coronary artery calcium in the PROMISE Study (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation. 2017;136(21):1993-2005
SCOT-HEART Investigators; Newby DE, Adamson PD, Berry C, Boon NA, Dweck MR, Flather M, et al. Coronary CT angiography and five-year risk of myocardial infarction. New Eng J Med. 2018;379(10):924-33
Adamson PD, Williams MC, Dweck MR, Mills NL, Boon NA, Daghem M, et al. Guiding therapy by coronary CT angiography improves outcomes in patients with stable chest pain. J Am Coll Cardiol. 2019;74(16):2058-70
Chang H-J, Lin Fay Y, Gebow D, An Hae Y, Andreini D, Bathina R, et al. Selective referral using CCTA versus direct referral for individuals referred to invasive coronary angiography for suspected CAD. JACC: Cardiovascular imaging. 2019;12(7_Part_2):1303-12
Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the evaluation and diagnosis of chest pain: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454
Lowenstern A, Alexander KP, Hill CL, Alhanti B, Pellikka PA, Nanna MG, et al. Age-related differences in the noninvasive evaluation for possible coronary artery disease: Insights from the prospective multicenter imaging study for evaluation of chest pain (PROMISE) trial. JAMA Cardiology. 2020;5(2):193-201
Chow BJW, Yam Y, Small G, Wells GA, Crean AM, Ruddy TD, et al. Prognostic durability of coronary computed tomography angiography. Eur Heart J Cardiovasc Imaging. 2021;22(3):331-8
Hochman JS, Anthopolos R, Reynolds HR, Bangalore S, Xu Y, O’Brien SM, et al. Survival after invasive or conservative management of stable coronary disease. Circulation. 2023;147(1):8-19
Nanna MG, Vemulapalli S, Fordyce CB, Mark DB, Patel MR, Al-Khalidi HR, et al. The prospective randomised trial of the optimal evaluation of cardiac symptoms and revascularisation: Rationale and design of the PRECISE trial. American Heart Journal. 2022;245:136-48
Dr Laura Murphy, Consultant Cardiologist and Lead in Integrated Care Cardiology, CHO91,2 1 Department of Cardiovascular Medicine, Mater Misericordiae University Hospital, Eccles Street, Dublin 7 2 School of Medicine, University College Dublin, Dublin 4











Leave a Reply
You must be logged in to post a comment.