NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Osteoporosis is a silent disease with no signs or symptoms to suggest a person is experiencing bone loss. This is why osteoporosis is known worldwide as ‘the silent killer’. No one feels bone loss, which is why patients must be screened for risk factors to prevent disease progression. Some 25 per cent of men and 50 per cent of women aged over 50 years will sustain a fracture due to osteoporosis. Many of these fractures will be preventable with the correct interventions.
Overview of osteoporosis
Most people have heard of the condition, but many are not aware of the horrific consequences that undiagnosed and untreated osteoporosis can bring, such as hip and other major fractures. These major fractures, in turn, present further risk of an array of additional complications. An estimated 20 per cent of people over-60 who fracture a hip will die within six-to-12 months due to complications like blood clots, pneumonia, and infection. A further 50 per cent will lose the ability to wash themselves, dress themselves, and walk across a room unaided. Some 84 per cent of those who fractured a bone in 2021 were admitted from home.
Some 90 per cent of total hip fractures are due to osteoporosis. The fact that only 19 per cent of patients are diagnosed with the condition is unacceptable, which is why every healthcare professional needs to know the basics of the disease and that it is preventable and treatable for most people. There is a significant amount of misinformation regarding osteoporosis in the public domain.
Common myths include:
A person cannot improve his/her bone health;
Osteoporosis only effects older women;
A calcium and vitamin D supplement is an osteoporosis treatment;
A DXA scan contains high doses of radiation;
People over-80 cannot be helped.
The Irish Osteoporosis Society (IOS), who are the national experts in bone health in Ireland, supports and guides sufferers towards an improved quality-of-life, and have even helped 88-year-olds in wheelchairs to regain their independence. A letter outlining the outcomes of one such example is outlined in Figure 1. The woman described had become wheelchair-bound due to multiple vertebral fractures when her son contacted the IOS. He had been told by three different healthcare professionals that nothing could be done to help his mother.
Dear Michele,
I wanted to thank your organisation for the help and guidance I received from you regarding my mum’s osteoporosis.
The improvement has been substantial and together with the practical steps we took to adapt her house, her quality-of-life has improved substantially, to the point that she is mobile and active again. We recently took her to Bath, UK, to celebrate her 90th birthday and she will go on a Mediterranean cruise with my sister next month! My Mum and I are extremely grateful for your guidance that has truly given her a new lease of life. Well done and keep up the great work.
Best Regards,
Vincent C
Figure 1: Letter from IOS service user
Causes of osteoporosis
There is a massive array of factors that contribute to osteoporosis development. Some of the 200 causes of bone loss includes family history (especially a fractured hip), steroids, eating disorders, low vitamin D levels, smoking, excess alcohol, over exercising, chemotherapy, radiation, drugs (including aromatase inhibitors for cancer, warfarin, heparin, some diuretics, some antidepressants, proton pump inhibitors, some medications for epilepsy, stroke, and paraplegia), high levels of stress, diabetes, being bed- or wheelchair-bound, coeliac disease, gluten and wheat sensitivity, lactose intolerance, cystic fibrosis, Crohn’s disease, irritable bowel syndrome, ulcerative colitis, and haemochromatosis. A massive range of factors contribute to the loss of bone density.
Skeletal changes
Many believe that as we age, it is normal to lose height and for posture to change as part of the ‘normal’ ageing process. People can indeed lose height due to wear and tear in the vertebrae and discs in their spine. However, it is very important that loss of height is investigated to ensure it is not due to undiagnosed osteoporotic fractures. It is also important to note that 75 per cent of people with vertebral fractures do not have constant pain. Many do experience initial back pain, but it generally progresses to become more intermittent in nature.
Signs and symptoms
The consequences of undiagnosed osteoporosis are often the only signs and symptoms of the disease. The most common presentations include:
Upper, middle, or lower back pain that is intermittent or constant;
Decreasing height;
Head beginning to protrude forward from the body;
Shoulders have become rounded;
A hump has started to develop on the back;
Development of a pot belly (not from excess food intake);
Body shape has changed.
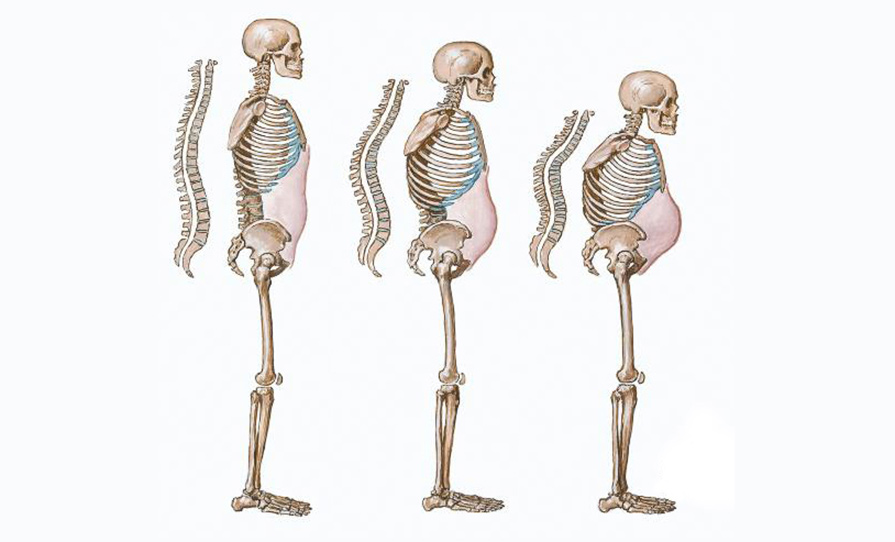
Figure 2: Skeletal progression in osteoporosis
The secondary effects on the vertebrae are not reversible. Figure 2 shows how vertebral wedge fractures can cause a Dowager’s hump to develop. This can happen at any age. The person’s head protrudes forward from the body, which causes the centre of gravity to shift. This places the patient at high risk of falling and falls usually result in further fractures. The ribs drop down as there is not enough bone in the spine to keep the person upright. The abdomen is pushed out and the rib cage ends up resting on the hip area. All these changes affect the person’s overall body shape, which can have a detrimental effect on self-image, mental health, quality-of-life, and independence.
Diagnosis
A dual energy x-ray absorptiometry (DXA) scan is similar to an x-ray, is completely painless and only takes 15 minutes. It contains only 10 per cent of the radiation of a regular chest x-ray. In fact, a flight from Dublin to New York results in more radiation exposure than a DXA. Repeat DXA scans should be done every two years at a minimum if bone loss has been diagnosed. It is an essential part of an overall treatment plan, for monitoring the person’s response to osteoporosis treatment, and to ensure they have not continued to lose bone, as bone loss is silent. Research shows that most fractures occur between a DXA scan T-score of -1.5 and -2.49, which indicates moderate-to-marked osteopaenia.
Management
How much a person can improve their bone health usually depends on the following:
How early the disease is diagnosed and treated;
The causes of bone loss;
If the causes of bone loss have been investigated and addressed;
If the person has taken the medication/ treatment prescribed;
If the person has/has not followed IOS recommendations, such as: “It is not safe for most senior citizens (especially those with bone loss) to lift children. Have your grandchild placed on your lap.”
If the person has continued or started an exercise programme that is not appropriate for those with bone loss, such as touching the toes. This can cause vertebral fractures for those with bone loss.
Exercise
When it comes to an exercise programme, everyone with bone loss should be progressed slowly to reduce the risk of fracture. The IOS does not recommend the following activities for those with bone loss, especially those who have vertebral fractures:
High impact exercise;
Heavy weights;
Trampolines;
Vibration machines;
Regular sit-ups;
Touching the toes (forward flexion);
Twisting of the back with the feet planted on the ground;
Yoga;
Riding a bike bent forward at the waist.
Calcium
Nutrition has a very important part to play in keeping bones healthy. Calcium, vitamin D, first-class proteins, and adequate calories are essential for bone and overall health. Older people need three servings of calcium per day, and if getting it from milk or yogurts, they should try to ensure that products are fortified with vitamin D. One serving of calcium is equal to:
A glass of milk;
An ounce (matchbox size) of cheese;
A carton of yogurt.
Tips to boost calcium intake include:
A bowl of breakfast cereal with milk;
Cheese on crackers or toasted cheese sandwich;
Fruit salad with yogurt;
Lasagne;
A fruit smoothie or milkshake;
Mug of hot chocolate;
Baked potato with grated cheese;
Pancakes;
Skimmed milk powder added to soups/ smoothies/sauces;
Porridge made with milk.
Vitamin D
Low levels of vitamin D reduces calcium absorption from the gut, triggering the secretion of parathyroid hormone (PTH) from the parathyroid glands. PTH stimulates the release of calcium from bones to maintain normal levels in the blood. Vitamin D and calcium levels should both be checked at least annually. The causes of bone loss also need to be investigated and osteoporosis should not be assumed. Absorption of vitamin D should also be assessed. It is important to be aware of malabsorption issues and gut disorders.
Anyone who cannot obtain their daily amount of vitamin D through food, or who is not in the sunshine regularly, should consider a vitamin D supplement. Not only is vitamin D essential for the absorption of calcium, but it is also crucial for healthy bones and it is vital for a healthy immune system. Low levels of vitamin D can also cause aches and pains all over, which can mimic the symptoms of fibromyalgia and can place a person at risk of multiple other diseases.
Facts about osteoporosis
There are many myths about osteoporosis and the following information is to dispel some of these myths and arm you with additional information:
Patients will not feel their bones getting weaker or stronger;
Those who eat healthily and exercise regularly can still develop osteoporosis;
Osteoporosis effects men and women of all age groups;
More men die from untreated osteoporosis than are diagnosed with prostate cancer;
More women die from complications of osteoporosis, such as fractures, than from cancers of the ovary, uterus, and cervix combined;
The most common bones to break first are the forearm, hip, and bones in the back, however, any bone can be affected;
Having an unhealthy skeleton puts patients at risk of losing their independence;
Prevention should start in utero;
There are 200 causes of bone loss, not just the menopause;
The causes of a person’s bone loss should never be assumed, and should always be investigated and addressed;
The biggest indicator of undiagnosed osteoporosis is breaking a bone from a trip and fall, even if it happened on cement, ice, or another harsh surface;
From age 75, a person is 25 times more likely to fracture a hip;
Currently, over €500 million is being spent in Ireland on treating broken bones;
Premature menopause (before 45 years), either natural or surgical, regular menopause, Depo-Provera contraceptive, irregular periods, loss of periods not due to pregnancy, and endometriosis are all high-risk factors for bone loss;
The risk of further broken bones is much higher in postmenopausal women who have already fractured;
The commonest cause of osteoporosis in males is hypogonadism, which may be the result of a variety of conditions, including abnormal chromosomes, infection of testes, mumps after puberty, and excessive physical or psychological stress;
Osteopaenia is the early stages of bone loss and should be investigated to prevent further bone loss;
50 per cent of women with vertebral fractures are undiagnosed;
It is very rare that exercise and nutrition alone can treat osteoporosis;
If physical education was made mandatory in schools, (part of the Junior and Leaving Cert curriculum), it would reduce the number of children at risk of osteoporosis, as well as many other chronic conditions, like obesity, diabetes, and mental health imbalances.
For further information about osteoporosis and the supports, resources, and services we provide, please contact the IOS, at 01 637 5050 or email: info@irishosteoporosis.ie. If you would like to be added to the notification list for our annual medical conference for health professionals on Saturday 19 October 2024, please email: events@irishosteoporosis.ie.











Leave a Reply
You must be logged in to post a comment.