NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Melanoma skin cancer – prevention and early diagnosis
By
Dr Una Kennedy, Dr Heather Byrne, Ms Aine Lyng & Ms Maria Greene
- 05th Jul 2022
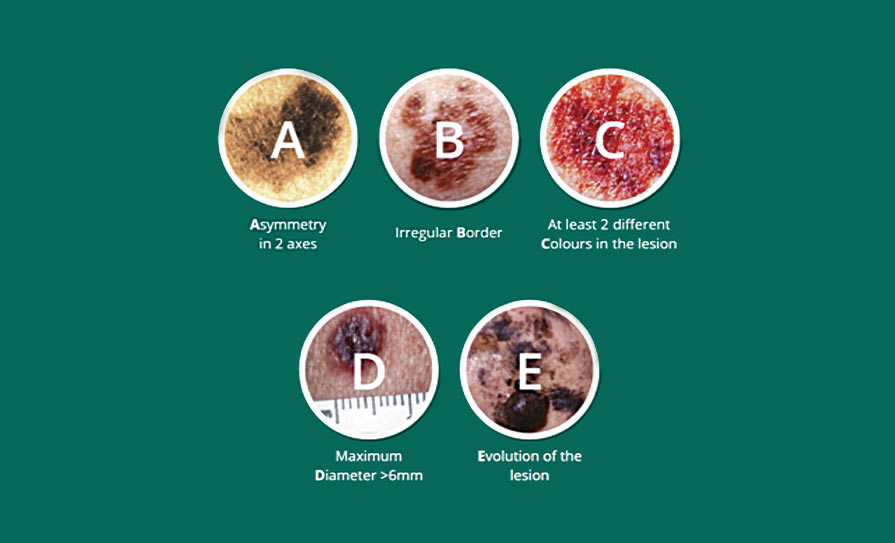
Figure 1: ABCDE lesion system for melanoma
Malignant melanoma, the most serious type of skin cancer, is the fifth most commonly diagnosed cancer in Ireland, accounting for one-in-20 new cancer cases.
Malignant melanoma, the most serious type of skin cancer, is the fifth most commonly-diagnosed cancer in Ireland (excluding non-melanoma skin cancer), accounting for one-in-20 new cancer cases. Every year, over 1,000 people in Ireland will be diagnosed with this disease, with males and females affected equally. The incidence of melanoma almost trebled between 1994 and 2017 in Ireland,1 and is expected to increase by 172 per cent between 2015 and 2045, potentially giving rise to 3,078 new cases of melanoma annually.2 Melanoma disproportionately affects younger age groups, with one-in-three cases (33 per cent) occurring in people under 50 years of age.3
Survival rates for melanoma skin cancer are high and it accounts for just 1.8 per cent of cancer deaths in Ireland, equating to approximately 170 deaths per year. Overall, 88 per cent of people diagnosed with melanoma are still alive 10 years after diagnosis. However, early diagnosis is strongly associated with improved survival; 97 per cent of people diagnosed with stage I melanoma are alive 10 years after diagnosis, compared to just one-in-two (48 per cent) people with stage IV disease.4
Risk factors for melanoma
Ultraviolet (UV) light
The single biggest risk factor for melanoma is exposure to ultraviolet (UV) light, such as sunlight or sunbed use. It is estimated that up to 90 per cent of cases of melanoma are caused by exposure to UV light. Sunlight comprises a number of wavelengths from infrared to UV light. UV rays, specifically UVA and UVB, are damaging to skin, causing DNA damage that can result in cancer.5 Sunburn, especially during childhood, is particularly harmful as it increases risk of melanoma later in life, but even non-burning, intermittent exposure to UV light can increase risk.
Exposure to UV light through use of sunbeds also increases risk. A recent study of 31 European Union (EU) and European Free Trade Association (EFTA) countries found that sunbed use accounted for approximately 5.1 per cent (n=4,450) of all newly-diagnosed cases of melanoma across these countries combined in 2012, with an associated economic cost of between €32.5-33 million.6
Skin type
The effects of UV exposure on skin are not the same for everyone. A person’s natural skin colour influences their risk of UV damage and skin cancer. Most people living in Ireland have fair skin (Fitzpatrick type I and II), which burns easily and tans poorly, placing them at increased risk of UV damage and skin cancer.
Family history
About 10 per cent of patients with melanoma skin cancer have a family history of melanoma.7 Risk is increased in people who have a first-degree relative (parent, sibling, child) who had melanoma at a young age (younger than 30 years). Carriers of BRCA 2 gene mutations have an increased risk of melanoma.
Other risk factors
Other risk factors for melanoma include:
A new or changing mole (this is the most important sign of a possible melanoma).
Atypical moles.
A large number of moles (>50).
A previous history of melanoma or other non-melanoma skin cancer.
Immunosuppression.
Melanoma prevention
Avoid exposure to UV light
Up to 85 per cent of melanoma skin cancers are due to exposure to UV radiation.8 UV rays are invisible and unlike infrared rays that cause heat, they cannot be seen or felt on our skin. The UV Index tells us how much UV radiation our skin is exposed to at any time. When the UV index is three or above, skin needs to be protected. Typically in Ireland, the UV index is three or above from April to September, even when it is cloudy. Limit time in the sun when UV rays are strongest; typically between the hours of 11:00am-3:00pm.
Wear protective clothing
Use of appropriate sun-protective clothing is one of the most important tools for sun protection. Cover skin as much as possible, wear long sleeves and collared t-shirts. To protect skin and eyes from UV radiation damage, wear a hat that protects the face, back of the neck, eyes and ears. Wide-brim, bucket, or legionnaire hats offer the best protection from UV radiation. Baseball caps are not recommended, as these styles do not protect the ears, cheeks or neck.
By adopting appropriate skin-protective behaviours, the majority of skin cancers caused by harmful UV radiation could be prevented
The European standard for sun protective clothing (EN 13758-2)9 stipulates a UPF (ultraviolet protection factor) greater than 40. For those garments that do not have a UPF label, some items will provide better sun protection than others:
Fabric that is tightly-woven and not transparent.
Clothing that gets wet or stretched may lose some of its protective qualities.
Dark clothes block more UV rays than light-coloured clothes.
Loose-fitting clothing is better because it is less likely to become stretched and allow UV light to penetrate. Remember to wear sunglasses with appropriate UV protection.
Use sunscreen
The ideal sunscreen would prevent 100 per cent of UV radiation from penetrating the skin and would provide long-term protection without the need for re-application. Unfortunately, such a sunscreen does not exist. Therefore, sunscreen alone is not sufficient to protect the skin, but should be used alongside other protective measures such as clothing and shade.
Sunscreen should be applied thickly and re-applied regularly (every two hours). Remember that water-resistant sunscreen can be rubbed off by clothing or towelling.
Sunscreens should provide protection against both UVB rays (indicated by the sun protection factor (SPF) rating) and also UVA rays (indicated by a star rating). Use a broad-spectrum sunscreen with an SPF of at least 30+ for adults and 50+ for children.
By adopting appropriate skin-protective behaviours, the majority of skin cancers caused by harmful UV radiation could be prevented.
Diagnosing melanoma early
Early diagnosis of melanoma is a critical first step in achieving higher survival rates and reducing treatment severity.
It is crucial that healthcare professionals and patients can recognise the early signs of melanoma. If a GP suspects that a patient has melanoma skin cancer they can refer that patient to a pigmented lesion clinic (PLC) or to a dermatology or plastic surgery service. The National Melanoma Referral Guidelines, available here www.hse. ie/eng/services/list/5/cancer/profinfo/resources/gpreferrals/national-melanoma-gp-referral-guidelines.pdf, aim to guide decision-making around which patients require referral.
Suspicious lesions which may require urgent referral include:
Any new or changing pigmented lesion.
A long-standing pigmented lesion which is changing progressively in shape, size or colour regardless of age.
A new pigmented line in a nail, especially where there is associated damage to the nail, or a lesion growing under a nail.
A pigmented lesion which has changed in appearance or which is persistently itching or bleeding.
An ‘ugly duckling’ pigmented lesion, which is one that looks different to all the other pigmented lesions that person has.
The ABCDE lesion system (Figure 1) can help to determine whether a mole or skin lesion is suspicious for melanoma.
Shave excisions and punch biopsies should not be carried out on naevi. If a patient presents with a suspicious pigmented lesion, the patient should be referred with the lesion intact to a consultant dermatologist or consultant plastic surgeon. If a melanoma has been inadvertently excised, the patient should be referred urgently to a consultant dermatologist or consultant plastic surgeon for multidisciplinary follow-up and care.
Resources for healthcare professionals
Currently, GPs in most regions in Ireland have access to PLCs. Patients should be referred to the PLCs using the electronic National Pigmented Lesion GP Referral Form. This form can be accessed via all of the four accredited GP computer software systems or by contacting Healthlink (www.healthlink.ie). If your region is not covered by a PLC, you can refer a patient with suspected melanoma to your local dermatology or plastic surgery service for urgent review.
The National Cancer Control Programme10 (NCCP) has developed two early detection of cancer modules, which are available free of charge to all healthcare professionals via HSeLanD, the HSE’s national online learning and development portal. These offer a valuable learning opportunity for melanoma and other skin cancers and are available at www.hseland.ie.
Resources on skin cancer prevention are also available at www.hse.ie/sunsmart/.
A significant proportion of melanoma cases are preventable by adopting skin protective behaviours. GPs and general practice nurses (GPNs) should take every opportunity to counsel patients about sun avoidance, sun protection, and early diagnosis of melanoma. GPs and GPNs are also encouraged to opportunistically assess patients attending their practice for signs of skin malignancy.
References
1. National Cancer Registry Ireland (NCRI). Cancer incidence statistics. (Accessed April 2022). www.ncri.ie/data/incidence-statistics
2. NCRI. Cancer incidence projections for Ireland 2020-2045 2019. www.ncri.ie/publications/cancer-trends-and-projections/ cancer-incidence-projections-ireland-2020-2045
5. Maslin DL. Do sunscreens protect us? Int J Dermatol. 2014 Nov;53(11):1319-23. doi: 10.1111/ijd.12606. Epub 2014 Sep 10
6. Krensel M, Schäfer I, Augustin M. Modelling first-year cost-of-illness of melanoma attributable to sunbed use in Europe. J Eur Acad Dermatol Venereol. 2019 Mar;33 Suppl 2:46-56. doi: 10.1111/jdv.15313
7. Goldman L, Schafer A (eds). Melanoma and non-melanoma skin cancers. Goldman-Cecil Medicine. 26th ed. Elsevier; 2029: 1344-50.e2
8. Cancer Research UK. Risks and causes of melanoma. www. cancerresearchuk.org/about-cancer/melanoma/risks-causes
9. Gambichler T, Laperre J, Hoffmann K. The European standard for sun-protective clothing: EN 13758. J Eur Acad Dermatol Venereol. 2006 Feb;20(2):125-30. doi: 10.1111/j.1468- 3083.2006.01401.x
10. Department of Health. National Cancer Strategy 2017-2026. 2017. www.gov.ie/en/publication/a89819-national-cancer-strategy-2017-2026/
Dr Una Kennedy, Gp Advisor To National Cancer Control Programme (Nccp); Dr Heather Byrne, Public Health Consultant, Nccp; Ms Aine Lyng, Cancer Prevention Officer, Nccp; And Ms Maria Greene, Cancer Prevention Officer, Nccp









Leave a Reply
You must be logged in to post a comment.