NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Multiple sclerosis: Diagnosis, management and impact of Covid-19
By
Dr Maria Gaughan, Aspire Fellow, Neurology Department, St. Vincent's University Hospital, Dublin
- 23rd Nov 2020
Multiple sclerosis nerve disorder and damaged myelin or MS autoimmune disease with healthy nerve with exposed fibre with scarrred cell sheath loss with 3D illustration elements.
MS overview
MS is a neurological condition caused by inflammation affecting the brain and spinal cord. It is a demyelinating disease, which pathologically is characterised by damage to the myelin. The exact aetiology remains unclear although a combination of genetic and environmental factors such as Epstein-Barr virus (EBV) exposure, vitamin D and smoking play a role.
First-degree relatives of those with MS are slightly more likely to develop the condition. MS is common in Ireland, with about 10,000 people affected and the incidence rate approaches one in 400.
It is typically diagnosed in young people, and there is a marked female preponderance. The increased utility of MRI imaging has likely led to diagnosis at an earlier stage of the condition than in the past. The clinical course typically begins with isolated relapses and almost complete recovery.
Within this period, radiological lesions can accumulate without any corresponding clinical signs. Progressive difficulties in walking emerge in almost 80-to-90 per cent of people with MS, although the time that this occurs following the onset of the illness can vary between 10 and 50 years.
Common initial presentations include optic neuritis; transverse myelitis; hemisensory symptoms; diplopia; and vertigo. Relapses can be quite subtle and difficult to identify, resulting at times in a delay in diagnosis.
Intravenous steroids are frequently given to shorten the duration of the relapse, but evidence suggests that they do not make a significant difference to the overall degree of recovery. In some centres, high-dose oral prednisolone at a dose of 1g/day is now given in certain situations, avoiding admission or repeated hospital attendances.
As outlined above, the mainstay in MS management is early initiation of appropriate disease-modifying therapy. This has changed significantly over the past 10 years, and our advice and management continues to evolve with changing evidence in the field.
The advent of the 2017 McDonald criteria has allowed an earlier diagnosis of MS – a single clinical event with imaging showing evidence of typical inflammatory lesions in more than one area usually associated with MS (periventricular, spinal cord, brainstem, pericallosal) and positive oligoclonal bands in the CSF, with exclusion of MS mimics will allow for a secure diagnosis.
MS medication has become increasingly personalised as we consider both disease factors and patient factors in choosing the medication in conjunction with the patient. One of the challenges in MS management is that we are frequently recommending a medication to people who feel very well, on the basis that evidence has demonstrated that in a large cohort of people with MS this will reduce the chance of further relapses and delay the time to disease progression. In choosing a medication with a patient, factors that are typically taken in to account include:
Severity of initial relapse;
Lesion load;
Lesion location >brainstem and spinal cord lesions are more likely to have clinical manifestations;
Potential complications of treatment.
Patient factors that are considered include:
Patient age;
Comorbidities;
Pregnancy planning;
Current work or school commitments;
Plans to travel;
Side-effect profile of medications;
Burden of monitoring;
Patient tolerance of risk.
The current availability of a wider range of treatment options has allowed us to make treatment decisions that are effective and palatable to people with MS. More recently treatment options have emerged for the previously neglected side of MS – progressive MS, which often manifests as an increased difficulty in walking.
It is typically irreversible, although progression can evolve slowly. Treatments are emerging on the market that aim to slow this progression. These include siponimod and ocrelizumab, although strict eligibility criteria remain. Activity is often defined as new radiological activity in a person with MS who is following a progressive course. The pivotal clinical trials of the medication suggest a slowing of progression of approximately 30 per cent over a two-year clinical trial.
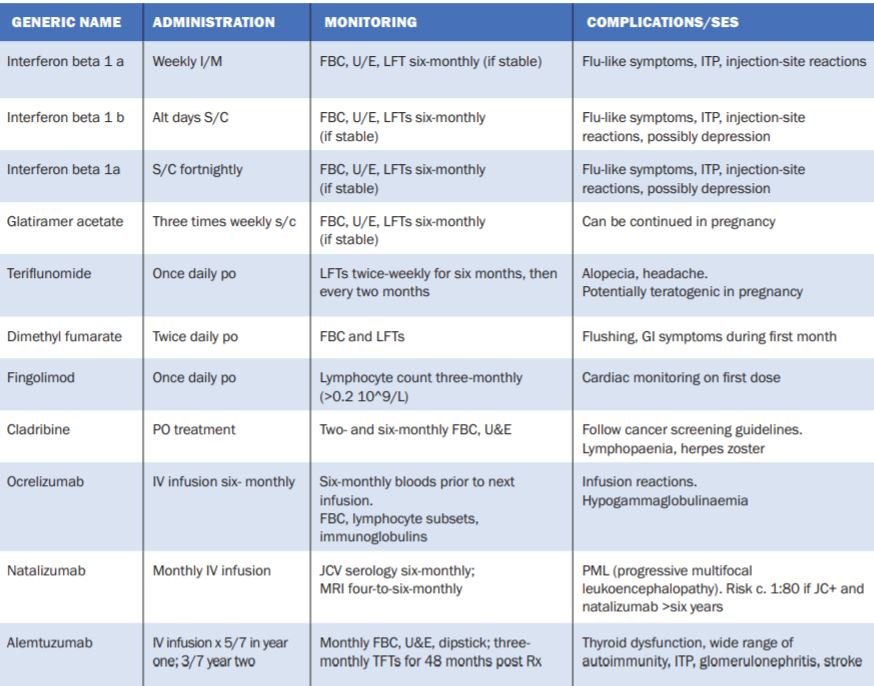
Table 1: Currently used disease-modifying treatments in MS
The effect was more pronounced in people with disease activity on imaging. A frustrating aspect of MS is that disease-modifying treatments appear to have a less pronounced impact on the condition in patients who are older. Ageing appears to also have an additive effect in progression.
Overall despite advances, there are significant unmet needs in the population with MS, particularly those who have a long history of the condition and those who are at a more advanced stage of disability. Clinical trials are beginning to focus on this population, for example, the O-HAND trial is designed to assess the impact of ocrelizumab on hand function in people with primary progressive MS.
Covid-19 and MS
As the implications of SARS-CoV-2 gradually dawned in Europe, rapid changes occurred in MS management across Europe. The degree to which people with MS, the majority of whom are on immunosuppressive or immunomodulatory medications, would be impacted was initially unclear.
Internationally, experts in the field attempted to categorise the risk of disease-modifying treatments based on mechanism of action of the medication and pathophysiological models of Covid-19. People with MS were advised to work from home, minimise social contacts and cocoon depending on the medication that they were taking. Clinic appointments were cancelled and switched to virtual appointments.
Medications considered to have a higher risk of immunosuppression, such as ocrelizumab and cladribine, were postponed. Patients due to commence these medications were rapidly worked up for an alternative. The goal at all times was to ensure effective control of MS, while minimising patient risk. Global registries were hurriedly established and have provided good data, although methodological issues remain.
Large French and Italian registries have provided interesting insights. People with MS are not at greater risk of catching Covid-19 than the general population. Indeed, due to the abundance of caution taken by people with MS, infection rates are likely lower than the general population.
The majority of medications taken by people with MS do not significantly increase the risk of severe infection resulting in hospitalisation, ventilation, ICU admission or death. There is a suggestion that caution should be exercised with ocrelizumab and rituximab, with studies suggesting increased risk of more severe infection, but not of death. The factors that increase risk of severe Covid-19 in MS appear to be age, disability and co-morbidities.
Current practices in Covid-19 have evolved to ensure that patients have, as far as is possible, access to neurology OPD with virtual OPD if this remains a preference. All services, both within the public and private systems, are attempting to deal with the backlog that arose during March and April. Timely access to disease-modifying treatments has remained a priority for the majority of patients.
If a patient with MS develops Covid-19 we would advise them to contact their MS team. They may require laboratory investigations to ensure they are not currently immune suppressed. They may require temporary suspension of their current treatment, although commonly treatment is continued.
As with other infections, they may experience a transient worsening of their MS symptoms, although these should improve with resolution of infection. We are attempting to collect data at a national level on people with MS who experience Covid-19 infection, in order to gain further insight into the degree of impact this may have.
Key points:
MS is a relatively common neurological disorder.
Common presentations include optic neuritis, transverse myelitis, sensory symptoms, oculomotor abnormalities, gait disturbance.
Clinical course is highly variable and difficult to predict at disease onset.
Early initiation of disease-modifying therapy is now strongly recommended based on clinical trial and epidemiological data.
Treatment of MS during pregnancy is now increasingly common, but should be carefully discussed prior to pregnancy with the treating neurology team.
Options for the management of progressive MS have emerged, but the treatment benefit remains modest.
Covid-19 and MS
Age, disability and co-morbidities are strongly correlated with more severe Covid-19 clinical course.
MS itself does not increase risk of severe Covid-19 infection, however as above, disability does.
Certain MS treatments can increase risk of more severe Covid-19 infection.
Ocrelizumab and rituximab have been associated with increased risk of hospitalisation and ICU admission, but not death in patients with Covid-19 infection. The increase in risk appears small.
Prolonged cocooning can potentially result in deconditioning and isolation in people with MS – closure of day services, difficulty in accessing physiotherapy services, and less ‘incidental’ mobility on a day-to-day basis. People with MS are encouraged to link in with online exercise classes such as those provided on the www.mstrust.org.uk website.
We also encourage regular walks/exercise and social contact with safe practices, such as mask wearing and frequent hand washing.
By
Dr Cara Martin, Associate Professor in Molecular Pathology, Cancer Prevention Research Theme Lead, Trinity St James’s Cancer Institute, Co-Lead of CERVIVA Research Consortium, School of Medicine, Trinity College Dublin
- 07th Apr 2025
By
Dr Karen Slattery, Postdoctoral Research Scientist, Trinity College Dublin, and Irish Cancer Society Research Awards 2025, Translational and Clinical Project of the Year Award winner
- 07th Apr 2025












Leave a Reply
You must be logged in to post a comment.