NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Review aims to implement a more personalised and multidisciplinary approach in treatment of menopause symptoms after cancer
Prof Donal Brennan, Professor of Gynaecological Oncology in the UCD School of Medicine, University College Dublin, and colleagues have published a new featured review on menopause treatment for cancer patients.
‘Managing menopause after cancer’ is part of a special series on menopause in The Lancet, and identifies the impact of early menopause and the severity of menopausal symptoms in cancer survivors, providing evidence-based recommendations following a review of the published literature and appraisal of professional guidelines. The article provides a comprehensive view of the current hormonal and non-hormonal therapy options studied and suggests a framework for more cost-effective and patient-focused models of care to meet the needs of a growing population of cancer survivors.
The article looks at a number of factors including patient cancer types, age, socio-economic status and cultural practices at play. It aims towards implementing a more personalised and multidisciplinary approach in treatment of menopause symptoms after cancer.
Prof Brennan, who is Principal Investigator in the Precision Oncology Ireland strategic partnership programme, as well as a gynaecological oncologist in the Mater Misericordiae University Hospital, Dublin, is one of the senior authors on the paper.
“Patients have repeatedly highlighted the burden of menopause symptoms after cancer treatment. They feel that these are often minimised or in some cases ignored,” said Prof Brennan. “We hope that this paper will provide a summary of evidence-based approaches to treat menopause symptoms, including the use of HRT if indicated, and, more importantly, stimulate more research in this area.”
Current challenges
The paper points out that cancer survival rates are continuing to improve and more women are experiencing long-term effects of cancer treatment, such as premature ovarian insufficiency or early menopause. The symptoms of these conditions can be significantly challenging to patients as they may be more severe than the symptoms of natural menopause.
In pre-menopausal women, treatment for common cancers, such as breast, gynaecological, haematological, and some low colorectal cancers, will often cause ovarian damage, potentially inducing permanent menopause. The standard of care for pre-menopausal high-risk oestrogen-receptor-positive breast cancer includes gonadotoxic chemotherapy followed by ovarian suppression plus oral endocrine therapy. This treatment can lead to more severe vasomotor symptoms (ie, hot flushes and night sweats) compared with natural menopause, particularly in younger women.
Diagnosing menopause after cancer can be challenging, as menopausal symptoms can overlap with other common symptoms in patients with cancer, such as fatigue and sexual dysfunction, the review document states. Many women resume menstruation within two years of chemotherapy completion; undetectable anti-Müllerian hormone at 30 months predicts menopause after chemotherapy for breast cancer and menopause is almost universal after ovarian radiation.
Managing menopausal symptoms after cancer can also be challenging and more severe than natural menopause, the authors note. Menopausal symptoms can extend beyond vasomotor symptoms. Treatment-induced symptoms might include sexual dysfunction and impairment of sleep, mood, and quality-of-life. In the long-term, premature ovarian insufficiency might increase the risk of chronic conditions, such as osteoporosis and cardiovascular disease. These symptoms can cause distress and impair quality-of-life and managing these symptoms is a leading priority for patients with cancer.
Patients with oestrogen-receptor-positive post-menopausal breast cancer are advised to take third-generation aromatase inhibitors (eg, anastrozole, letrozole, and exemestane), which can induce or aggravate menopausal symptoms, including hot flushes, night sweats, and vaginal dryness.
Peri-menopausal or post-menopausal women diagnosed with oestrogen-receptor-positive cancers, while taking menopausal hormone therapy (MHT) will be advised to stop, which can cause resurgent vasomotor symptoms that are further exacerbated by anti-oestrogen therapy, the paper notes.
Menopausal symptoms are a common reason for not starting or prematurely stopping endocrine therapy, which directly increases morbidity and mortality from breast cancer. Newer protocols extending endocrine therapy from five-to-10 years in oestrogen-receptor-positive or progesterone-receptor-positive cancer are likely to increase the burden of symptoms.
In a 2021 community-based survey (n=385), the prevalence of menopausal symptoms in survivors of breast cancer six years after diagnosis was high: Some 346 (90 per cent) had vasomotor symptoms or sleep disturbance, 289 (75 per cent) had vaginal dryness, 240 (62 per cent) had mood swings, and 229 (59 per cent) had sexual difficulties. Severity of hot flushes and sleep disturbance predicted their inability to resume everyday activities. Less than a third were offered treatment and less than half found this to be effective.
Key treatment advice points include:
MHT is an effective treatment for vasomotor symptoms and seems to be safe for many patients with cancer, the paper states.
Women younger than 45 years without contraindications should be offered an individualised treatment plan including MHT after cancer treatment.
If MHT is contraindicated, non-pharmacological and non-hormonal treatments are available for vasomotor symptoms; vaginal oestrogen seems to be safe for most patients with cancer and growing evidence supports safety after breast cancer.
Multidisciplinary management of menopause after cancer is essential and should include primary care and, if appropriate, allied health practitioners.
Reaching the population who need treatment is a global problem and online platforms are being developed to better support and empower patients with cancer to make shared, evidenced-based decisions with their local healthcare provider.
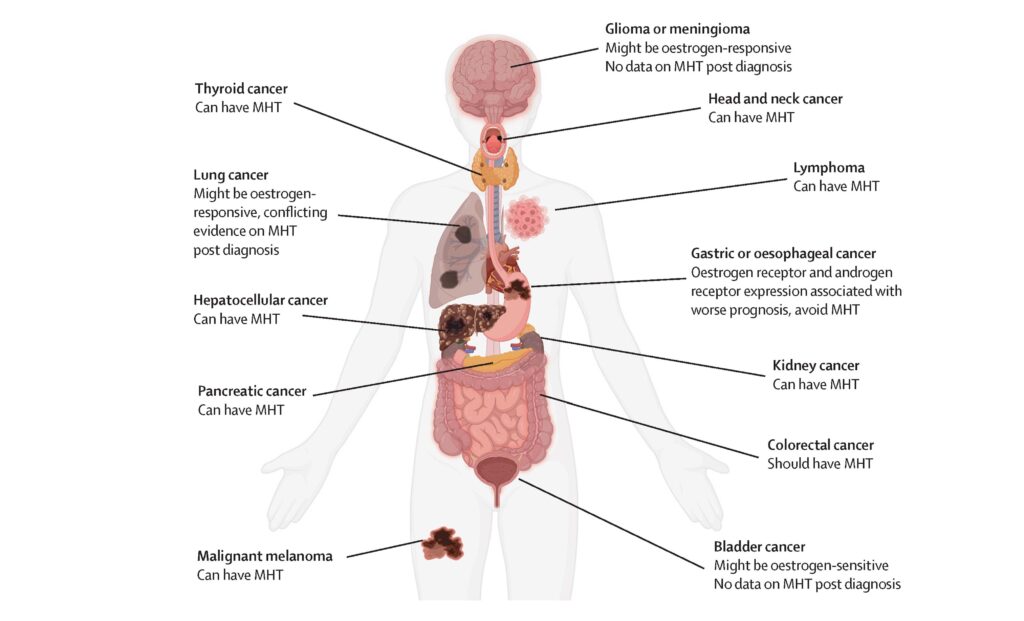
Figure 1: Use of MHT after non-female specific cancers. Source: Hickey M, et al. Managing menopause after cancer, 2024. The Lancet
Evidence gaps
Almost all published studies on menopause and cancer are in early breast cancer and less is known about advanced breast cancer or other cancers in women, the paper acknowledges. There are no reliable ways of predicting who will experience severe or prolonged menopausal symptoms following cancer treatment.
In breast cancer, vaginal dryness is more common with aromatase inhibitors than tamoxifen and some evidence suggests that switching between tamoxifen and aromatase inhibitors can improve vasomotor symptoms in post-menopausal women, the authors state.
Among pre-menopausal women, switching to tamoxifen plus ovarian function suppression or tamoxifen alone might improve vaginal dryness, and this treatment can be considered by the treating oncologist when weighing the advantages and disadvantages of disease risks and tolerance of therapy.
Decisions regarding the necessity and type of hormonal therapy used for breast cancer treatment depend on menopausal status, evolving literature, disease risk, and patients’ comorbidities, tolerance over time, and preferences.
Many patients have inadequate centralised care for managing menopausal symptoms after cancer treatment and more information is needed about cost-effective and patient-focused models of care for this growing population, the article concludes.
Reference Hickey M, Basu P, Sassarini J, Stegmann ME, Weiderpass E, Nakawala Chilowa K, Yip CH, Partridge AH, Brennan DJ. Managing menopause after cancer. Lancet. 2024 Mar 9;403(10430):984-996. The full paper is available at: www.thelancet.com/series/menopause-2024












Leave a Reply
You must be logged in to post a comment.