NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Dr Anna Witkowska and Prof Geraldine M McCarthy
- 05th Feb 2024
Gout is a chronic inflammatory process that requires lifelong treatment and is associated with an increased burden of cardiovascular co-morbidities and higher mortality
Case report
An 82-year-old man was admitted with a four-day history of left hand and wrist pain that had not improved with paracetamol. On examination, the left hand was swollen, erythematous, and tender to touch. There was evidence of non-tender subcutaneous nodules over the finger pads.
Past medical history included congestive heart failure, hypertension, atrial fibrillation, anaemia under investigation, ischaemic heart disease, and recurrent urinary tract infections. Regular medication included lipid-lowering therapy, multivitamins, diuretics, an anticoagulant, and a proton pump inhibitor.
Inflammatory markers were raised, and prompt antibiotic treatment was initiated by the admitting doctor for presumed cellulitis. Due to lack of response to treatment, antibiotics were switched to oral prednisolone and colchicine with improvement of symptoms and clinical markers. A diagnosis of tophaceous gout was made. Of note, serum uric acid levels were elevated – 639umol/L (177-465umol/L).
Treatment was complicated by development of excessive agitation, which was assumed to be secondary to prednisolone that was subsequently stopped. Colchicine was discontinued due to ongoing diarrhoea. Non-steroidal anti-inflammatory drugs (NSAIDs) were contraindicated due to the use of anticoagulation. The patient was initiated on an interleukin-1 (IL-1) inhibitor, anakinra, with good response without any major side-effects. He was commenced on a maintenance allopurinol treatment that was guided by the serum uric acid levels. Due to the burden of the disease and intolerance to different pharmacological agents, the patient suffered with recurrent gout flares requiring multiple hospitalisations. This case illustrates the difficulty of diagnosing and managing gout. Initially, the admitting physician was concerned about an acute infection and prescribed an antibiotic. The diagnosis was eventually made by synovial fluid aspiration and examination under polarised light microscopy when multiple intra- and extra-cellular negatively birefringent crystals were identified. The subcutaneous nodules were in fact gouty tophi. Gout flares typically develop acutely and present with erythema, swelling and pain, which may mimic infection. Treatment of gout should be tailored to the patient, taking into consideration potential treatment complications.
Gout is the most common form of inflammatory arthritis. Earliest descriptions of gout date back to the fifth Century BC. It used to be known as ‘the disease of kings’ due to its association with certain foods and alcohol.
The prevalence of gout is highly variable among different ethnic groups, suggesting that both genetic and environmental factors play a role in its pathogenesis. Based on North American, European, and Asian studies, the prevalence ranges between <1-and-6.8 per cent in adults.1
The highest prevalence is reported in Oceania – up to 13.9 per cent of Pacific people living in New Zealand have gout.2
Gout is more common in men than women; with a male-to-female ratio of 2:1-to-4:1.3 Testosterone inhibits, while oestrogen promotes, urate excretion by the kidneys. It is therefore uncommon for women to develop gout before menopause. However, with increasing age, the male-to-female ratio decreases.4
Gouty arthritis is correlated with many co-morbidities. Various epidemiological studies have shown that it is associated with hypertension, hyperlipidaemia, chronic kidney disease (CKD), and increased cardiovascular risk.5 Thus, perhaps unsurprisingly, it is associated with increased mortality, probably due to the burden of co-morbidities.6
Risk factors
There is a proven correlation related relationship between the levels of uric acid and the risk of gout. Interestingly, other animals do not develop hyperuricaemia due to an enzyme called uricase that converts uric acid to soluble allantoin, which is then easily excreted. Humans and other primates have lost this enzyme during our evolution; thus, our species is prone to gout.7
Uric acid is a breakdown product of purines (DNA, ATP turnover). Thus, its levels can be increased in conditions with high cellular production of purines or high purine oral intake. Serum uric acid levels will also be high in conditions with decreased uric acid excretion. One-third of uric acid is excreted by the gut, and two-thirds by the kidneys.
One-third of uric acid is excreted by the gut, and two-thirds by the kidneys
High cellular production of purines can be found in disease processes that result in rapid cell turnover, such as malignancy, psoriasis, or tumour lysis syndrome. Likewise, high ATP turnover will result in increased uric acid levels in sepsis, myocardial infarction, or seizures.
High purine intake can also result in increased uric acid levels. Meat and seafood have a high purine content.
There are other mechanisms by which food can increase serum uric acid levels. For instance, consuming sugary drinks high in fructose will lead to increased ATP turnover and hyperuricaemia.
Alcohol increases uric acid levels in the body by several means, including increased ATP turnover and decreased uric acid excretion by the kidneys. Also, some types of alcohol (eg, beer) have high purine content.8
Despite all the above, the role of diet in the development of gout is controversial – studies have found that the type of diet has little effect on the serum urate concentration levels in healthy populations.9
Clinical signs and symptoms
The renowned English physician, Thomas Sydenham, gave an accurate description of an acute gout flare based on his own experience: “The victim goes to bed and sleeps in good health. About 2 o’clock in the morning he is awakened by a severe pain in the great toe; more rarely in the heel, ankle or instep. The pain is like that of a dislocation, and yet the parts feel as if cold water were poured over them. Then follows chills and shiver with a little fever. The pain, which was first moderate, becomes more intense.”
Indeed, gout flares typically occur between midnight and 5am. They are characteristically acute and very painful, with erythema, swelling, and tenderness of the affected joints. The first metatarsophalangeal (MTP) joint is the most common site, being involved in 50 per cent of the first acute flares. Other common sites include the ankles, knees, and toes.10 Acute attacks are self-limiting and last anything from one-to-two weeks. They can be associated with a fever, especially if more than one joint is affected.
Untreated persistent hyperuricaemia can lead to more frequent and severe attacks, which can become polyarticular. Interestingly, gout initially presents as a polyarticular attack in 10 per cent of cases.11
Tophaceous gout is characterised by tophi formation – these are depositions of monosodium urate crystals in joints and soft tissues. They typically affect olecranon bursa, fingers, toes, Achilles tendon, or even the helix of the ear. They are composed of gouty crystals surrounded by inflammatory cells. Tophi are particularly difficult to treat, as they constitute a reservoir of urate in the body. Lowering serum uric acid levels will lead to a shift in the equilibrium of the total body urate burden and release of more uric acid from the tophi reservoir.
Tophi are associated with bone and joint damage. Deposition of urate crystals lead to chronic inflammatory response with local production of pro-inflammatory interleukins and metalloproteinases together with an activation of synovial fibroblasts and osteoclasts. This leads to tissue damage and remodelling resulting in bone destruction. In addition, the mass effect of the tophus itself can lead to joint damage.12 This can be seen on plain x-ray as the characteristic ‘punched out lesions’.
Differential diagnosis
There are many gout mimics that physicians should be aware of. Septic arthritis also presents with acute swelling, erythema, and tenderness. Ideally, fluid aspirate should be examined for crystals as well as for fluid white cell count and gram stain.
Acute calcium pyrophosphate (CPP) deposition disease (‘pseudogout’) can clinically resemble gout. However, it is associated with a different joint involvement pattern with wrists and knees being commonly affected. Plain x-rays can reveal chondrocalcinosis. Synovial fluid examination will reveal CPP crystals. Monosodium urate (MSU) and CPP crystals can co-exist.
Gout diagnosis – clinical investigations
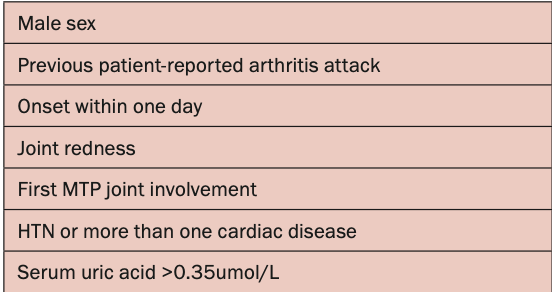
The gold standard of diagnosis is the microscopic analysis of synovial fluid or tophi. MSU crystals are needle shaped and negatively birefringent under polarised light. Synovial fluid should be sent for cell count, culture and sensitivity and gram stain, as gout and septic arthritis can co-exist. However, if the fluid examination is not possible, there are certain diagnostic criteria that can be used. The Acute Gout Diagnosis Rule was developed to stratify the risk for gouty arthritis. These criteria include certain features that are more likely to be attributed to gout (Table 1).13
Table 1: Features typical for gouty arthritis as per the Acute Gout Diagnosis Rule
Serum urate concentrations can be normal in a flare due to increased renal excretion, and thus can represent a negative acute phase reactant. Hyperuricaemia occurs in 20 per cent of males and 4 per cent of females in the general population and on its own is insufficient for a diagnosis of gout.14 Inflammatory markers, such as C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR), will be elevated during an acute flare, however, these are non-specific findings.
Recently, the role of fibrinogen in monitoring disease activity in patients with gout has been supported by several studies. Fibrinogen was found to be a more specific marker of an acute flare than other conventional inflammatory indicators. It is believed that increased levels of fibrinogen are caused by activation of the coagulation system following damage to vascular endothelial cells during a flare.15
Ultrasonography and dual-energy CT scans aid in diagnosis of gout.16,17 Ultrasonographic findings include ‘double contour sign’ (MSU crystal deposition on the surface of hyaline articular cartilage) and intra-articular tophi. Nevertheless, absence of MSU crystal deposition on ultrasound or dual aspect CT does not exclude gout, especially in the early phase of the disease. X-rays can reveal punched out lesions with sclerotic margins and overhanging edges. Plain radiographs are also normal at the time of initial diagnosis.
Treatment
Treatment of gout can be divided into treatment of acute flares and chronic management.
The goal of treatment of an acute flare is pain control and suppression of inflammation. This can be achieved with either prednisolone, NSAIDs, or colchicine. Studies have shown equivalent efficacy of oral agents and thus treatment choice depends on patient preferences, co-morbidities, and costs.18,19
For instance, NSAIDs are not recommended in the setting of peptic ulcer disease, kidney or cardiac disease, or anticoagulant use. High-dose steroids should be avoided in infection or diabetes. Colchicine toxicity can occur with kidney or liver disease. Moreover, use of other medications such as ketoconazole, cyclosporin or clarithromycin can potentiate colchicine toxicity.20 The most common side-effect of colchicine is diarrhoea.
Recent trials have found that the use of colchicine may decrease the rate of cardiovascular events in high-risk populations.21,22 The 2021 European Society of Cardiology guidelines recommend the use of low-dose colchicine (0.5mg daily) as secondary prevention of cardiovascular disease in this patient group if other risk factors are not controlled.23
Serum urate concentrations can be normal in a flare due to increased renal excretion, and thus can represent a negative acute phase reactant
Interleukin-1 plays a central role in the inflammatory process driving gouty arthritis. Indeed, IL-1 inhibitors have been found to be useful in acute gout management. Anakinra, an IL-1 inhibitor which is delivered via the subcutaneous route, has been found to have a similar safety profile and efficacy to other therapies for acute flares.24
Long-term management of gout
It is important to highlight to all patients presenting with an acute gout flare that long-term urate lowering therapy (ULT) prevents future flares and joint damage. There are three different classes of urate-lowering drugs. Xanthine oxidase inhibitors (allopurinol, febuxostat) hinder uric acid production. Uricosurics (probenecid, lesinurad) promote uric acid excretion by the kidneys. Recombinant uricases (pegloticase) convert uric acid to soluble allantoin.
ULT is generally recommended to individuals with two or more acute flares, or one or more flare in the presence of co-morbidities (CKD, urolithiasis, very high serum urate levels).
ULT can be started during the attack if the inflammation is adequately treated. Treatment should not be discontinued during an acute attack. Flares tend to occur at an increased frequency following initiation of ULT, and thus anti-inflammatory agents, such as colchicine or NSAIDs, should be continued for at least three-to-six months to prevent further attacks.25
Long-term treatment of gout is guided by the ‘treat to target’ approach. Typically, the initial dose of allopurinol is 100mg/day or 50mg/day in CKD. The dose can be slowly titrated based on the uric acid level up to a maximum 900mg/day. Serum uric acid target levels should be below 360umol/L for most patients, but less then 300umol/L in tophaceous gout. If allopurinol is not tolerated or serum target urate levels are not achieved, other agents should be considered.
Allopurinol-associated rash requiring withdrawal of the drug occurs in 1-to-2 per cent of patients. Allopurinol hypersensitivity syndrome, which occurs in the first few months after treatment initiation, is a rare, life-threatening reaction that involves widespread cutaneous changes and acute kidney injury in the presence of eosinophilia.26 Patients of South East Asian descent are at higher risk, and the condition is associated with HLA-B*58:01 allele.25 Other risk factors include CKD and high initial doses of allopurinol.27
Febuxostat, a potent non-purine xanthine oxidase inhibitor, received a black box warning by the US Food and Drug Administration for an increased risk of cardiovascular events. This move, however, has been controversial. A 2020 European Medicines Agency study showed no evidence of an increased risk of major cardiovascular events with febuxostat compared to allopurinol.28
Conclusions
Gout is not only a disease of the joints; it is a chronic inflammatory process that requires lifelong treatment and is associated with an increased burden of cardiovascular co-morbidities and higher mortality overall. Fortunately, we have effective treatments for both acute flares and long-term management. It is imperative to educate our patients and their healthcare providers about the potential long-term complications of gout and highlight the role of lifelong ULT.
References
Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: Prevalence, incidence, treatment patterns, and risk factors. Nat Rev Rheumatol. 2020 Jul;16(7):380-390
Dalbeth N, Dowell T, Gerard C, et al. Gout in Aotearoa New Zealand: The equity crisis continues in plain sight. N Z Med J. 2018 Nov 9;131(1485):8-12
Kuo CF, Graigne MJ, MAllen C, et al. Rising burden of gout in the UK, but continuing suboptimal management: A nationwide population study. Ann Rheum Dis. 2016 April;74(4):661-667
Harrold LR, Yood RA, Mikuls TR, et al. Sex differences in gout epidemiology: Evaluation and treatment. Ann Rheum Dis. 2006 (65)10:1368-1372
Stamp LK, Chapman PT. Gout and its comorbidities: Implications for therapy. Rheumatology (Oxford). 2013;52(1):33-44
Kim SY, De Vera MA, Choi HK. Gout and mortality. Clin Exp Rheumatol. 2008 Sep-Oct;26(5 Suppl 51):S115-119
Alvarez-Lario B, Macarron-Vincente J. Uric acid and evolution. Rheumatology (Oxford). 2010 Nov;49(11):2010-2015
MacFarlane LA, Seoyoung CK. Gout: A review of non-modifiable and modifiable risk factors. Rheum Dis Clin North Am. 2014 Nov; 40(4):581-604
Major TJ, Topless RK, Dalbeth N, Merriman TR. Evaluation of the diet wide contribution to serum urate levels: Meta-analysis of population-based cohorts. BMJ. 2018 Oct 10;363:k3951
Coburn BW, Mikuls TR. Treatment options for acute gout. Fed Pract. 2016 Jan;33(1):35-40
Rothschild BM, et al. Gout and pseudogout clinical presentation. Medscape. 2023 Mar 23. Available at: https://emedicine.medscape.com/article/329958-clinical
Dalbeth N, Pool B, Gamble GD, et al. Cellular characterisation of gouty tophus, a quantitative analysis. Arthritis Rheum. 2010 May;62(5):1549-1556
Janssens HJEM, Fransen J, Van de Lisdonk EH, et al. A diagnostic rule for acute gouty arthritis in primary care without joint fluid analysis. Arch Intern Med. 2010;170(13):1120-1126.
Chen-Xu M, Yokose C, Rai SK, et al. Contemporary prevalence of gout and hyperuricaemia in the United States and decadal trends: The National Health and Nutrition Examination Survey, 2007-2016. Arthritis Rheum. 2019 Jun;71(6):991-999
Chen S, Huang X, Huang Y, et al. Role of plasma fibrinogen in assessing disease activity of patients with gout. Clinica Chimica Acta. 2020 Nov;510:483-487
YH Lee, GG Song. Diagnostic accuracy of dual-energy computed tomography in patients with gout: A meta-analysis. Semin Arthritis Rheum. 2017;47:95-101
YH Lee, GG Song. Diagnostic accuracy of ultrasound in patients with gout: A meta-analysis. Semin Arthritis Rheum. 2018;47:703-709
Janssen HJ, Janssen M, van de Lisdonk EH, et al. Use of oral prednisolone or naproxen for the treatment of gout arthritis: A double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860
Roddy E, Clarkson K, Blagojevic-Bucknall M, et al. Open label randomised pragmatic trial (CONTACT) comparing naproxen and low-dose colchicine for the treatment of gout flares in primary care. Ann Rheum Dis. 2020;79:276-284
Terkeltuab RA, Furst DE, Digacinto JL, et al. Novel evidence-based colchicine dose-reduction algorithm to predict and prevent colchicine toxicity, in the presence of cytochrom P450 3A4/P-glycoprotein inhibitors. Arthritis Rheum. 2011;63:2226-2237
Tardif JC, Kouz S, Waters DD, et al. Efficacy and safety of low dose colchicine after myocardial infarction. N Engl J Med. 2019;381:2497-2505
Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383:1838-1847
Visseren FLJ, Mach F, Smulders YM, et al. ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227-37
Janssen CA, Oude Voshaar MAH, Vonkeman HE, et al. Anakinra for the treatment of acute gout flares: A randomised, double-blind, placebo-controlled, active comparator, non-inferiority trial. Rheumatology (Oxford). 2019;58:1344-1352
Fitzgerald JD, Dalbeth N, Mikuls T. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020 Jun;72(6):744-760
Gutierrez-Macias A, Lizarralde-Palacios E, Martinez-Odriozola P, et al. Fatal allopurinol hypersensitivity syndrome after treatment of asymptomatic hyperuricaemia. BMJ. 2005;331:623-624
Stamp LK, Taylor WJ, Jones PB, et al. Starting dose is a risk factor for alloprinol hypersensitivity syndrome: A proposed safe starting dose of allopurinol. Arthritis Rheum. 2012;64:2529-2536
MacKenzie IS, Ford I, Nuki G, et al. Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): A multi-centre, prospective, randomised, open-label, non-inferiority trial. Lancet. 2020;396:1745-1757
Dr Anna Witkowska, Rheumatology Registrar, Mater Misericordiae University Hospital, Dublin; and Prof Geraldine M McCarthy, Full Clinical Professor of Medicine, School of Medicine and Medical Science, University College Dublin, and Consultant Rheumatologist, Mater Misericordiae University Hospital, Dublin












Leave a Reply
You must be logged in to post a comment.