







DR DAVID BUCKLEY, FRCGP, MICGP, Medical Director of the Kerry Skin Clinic, Tralee, Co Kerry, www.kerryskinclinic.ie
Acne is probably the most common dermatology problem seen in general practice, yet many patients still struggle to manage their acne.
Acne is a very common, chronic inflammatory skin disease. It occurs in 90 per cent of teenagers and half of them continue to have acne as adults. About 20 per cent of young people experience moderate or severe acne.
Acne is probably the most common dermatology problem seen in general practice. The diagnosis is usually obvious and the treatment for the majority of patients is simple and straightforward. Despite this, many patients still struggle to manage their acne, which occurs on the worst part of their body (face) at the worst time of their life (teenagers and young adults). Left untreated or partially treated, acne may lead to physical and/or psychological scarring.
Pathophysiology
Acne is a disease of the pilosebaceous unit. There are four major contributing factors (Table 1). It usually occurs at puberty or in early adult life when there is a surge of hormones. Patients with acne do not usually have too much or too little hormones (apart from those with polycystic ovary syndrome (PCOS)).
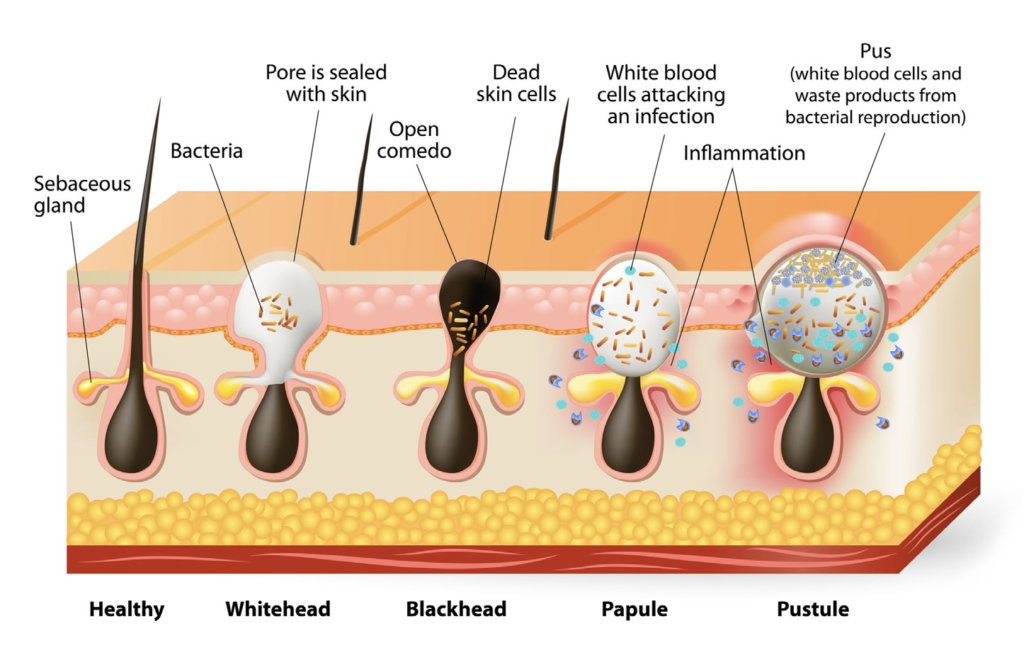
The problem with acne sufferers is end-organ hypersensitivity to the normal fluctuations in hormones that occur at this time of life and this may be genetically determined. This causes the pilosebaceous unit to over-produce oil, leading to blocked pores called ‘comedones’. Comedones may be almost invisible (micro-comedones), closed comedones (whiteheads), or open comedones (blackheads). These comedones become colonised by the commensal bacteria known as Cutibacterium acnes (C. acnes), which causes inflammation in the area, resulting in the inflammatory features of acne such as papules, pustules, cysts or nodules (Photo 1 and Figure 1).
| THERE ARE FOUR MAIN MECHANISMS IN THE AETIOLOGY OF ACNE: |
| A. Excessive production of sebum (under hormonal control) |
| B. Follicular plugging causing micro-comedones and comedones |
| C. Overgrowth of micro-organisms especially C. acnes (formerly Propionibacterium acnes), which causes release of inflammatory cytokines |
| D. Inflammation causes the pylosebaceous cyst wall to rupture, resulting in an intense foreign body-like reaction, which leads to further development of inflammatory lesions (papules, pustules, nodules, cysts) |


Treating the inflammatory features of acne with oral or topical antibiotics without treating the underlying problems of excess oil and comedones will only partially help and the patient will relapse quickly once the treatment is stopped.
Topical treatments
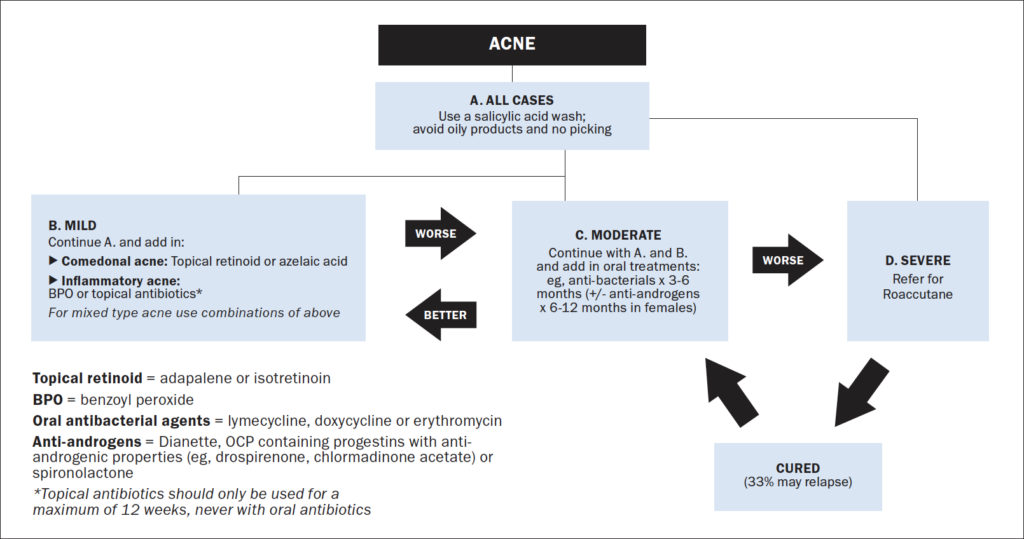
The first-line treatment for acne sufferers should be to tackle the excess oil and comedones (Photo 2). Acne washes containing salicylic acid, 0.5-to-2 per cent, may help. However, most patients will also need a topical retinoid such as topical isotretinoin (eg, Isotrex), or a retinoid-like agent such as adapalene (eg, Differin Gel), or a combination of a retinoid-like agent such as adapalene with benzoyl peroxide (eg, Epiduo).
These topical agents can be irritating and patients need careful counselling on how to use them properly. These products should be put all over the acne-affected areas and not just onto the individual spots since they are designed to reduce oil production, prevent the build-up of comedones, and avoid the development of papules and pustules. These agents should be applied sparingly on alternate nights for the first week or two until the patient gets used to the drying effects before increasing to nightly use.
Some patients may need to use a lightweight, non-greasy, non-comedogenic moisturiser in the morning to counteract the drying effects of topical retinoids or retinoid-like agents.
Patients with sensitive skin or a history of eczema may not be able to tolerate these topical agents and may have to try a less irritating topical treatment such as azelaic acid 20 per cent (Skinoren Gel) instead.
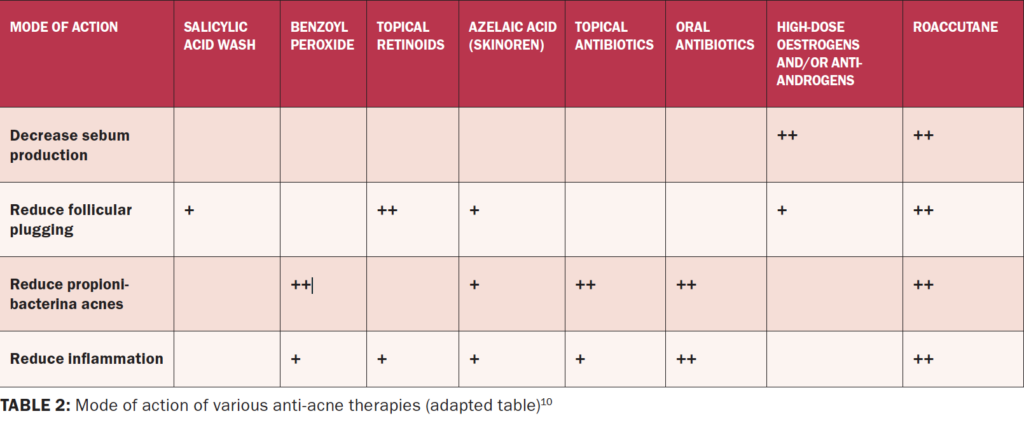
These topical retinoids and retinoid-like agents are very slow to work. It can take weeks or months to see an improvement in the acne. Results can be enhanced by logical combinations such as a topical retinoid or a retinoid-like agent in association with an anti-inflammatory agent such as benzoyl peroxide (BPO) or antibiotics either topically or orally (Table 2).
BPO, like topical retinoids and retinoid-like agents, can be quite irritating and should be used sparingly and on alternate days initially before increasing to daily use. Because BPO is cheap and available without prescription it is sometimes used first-line on its own with an anti-acne wash when there is primarily inflammatory acne without too much oiliness or comedones. BPO is also useful as it does not make the patient sensitive to sunlight and it can be used in pregnancy. In addition, it can be useful for treating large areas such as the back and chest as it comes in relatively large tubes (eg, Acnecide Gel 60 grams). Apart from its drying effects, the other disadvantage of BPO is that it can bleach clothing so it is best to advise patients to apply it at night and if they are putting it on their chest or back they should use a white T-shirt at night, white sheets, white pillowcases, and white towels.
BPO does not have any anti-comedonal effects so it is best used in combination with topical retinoids or retinoid-like agents for more moderate-severity acne, especially if there are many comedones.
For most patients with acne, combining BPO with adapalene (a retinoid-like agent) such as Epiduo Gel is very convenient as it only has to be applied once at night all over the acne-affected areas of the face and neck. However, this combination of two potentially irritating agents can be drying and somewhat irritating, especially at the start of treatment. Applying it alternate nights for the first week or two can help with the irritation and most patients can then increase up to nightly use. One bottle (45g) should usually last two-to-three months when applying it to the face. If this combined agent causes too much irritation it might be necessary to apply a topical retinoid or retinoid-like agent such as topical isotretinoin or adapalene at night and BPO in the morning, but this involves twice-daily treatments, which may reduce compliance, especially in men.
BPO can have as good an anti-bacterial effect on acne as topical antibiotics without the risks of developing resistance. It has the advantage over topical antibiotics in that it can be used long-term for weeks, months or years without losing its effect.
Patients with more moderate to severe acne may need an antibiotic added to the above mentioned topical treatments to get the acne under control (Table 3). While topical antibiotics offer some anti-bacterial effects, resistance can develop quickly and they are only licensed to be used for three months, which is a very short time in an acne sufferer’s life. Acne can lasts years, not months, so topical antibiotics have a very limited role in the overall management of acne.
Systemic treatments
Oral antibiotics used for a maximum of three-to-six months have useful anti-bacterial effects, but products such as lymecycline 405mg daily or doxycycline 100mg daily also have powerful anti-inflammatory effects, which is probably their primary mechanism of action in acne. However, like BPO, antibiotics have no anti-comedonal effects, so they should never be used alone to treat acne. It is best to combine antibiotic treatments with anti-comedonal treatments such as topical retinoids or retinoid-like agents. The combination of a topical retinoid or a retinoid-like agent with an oral antibiotic for three-to-six months should clear up 90 per cent of acne in 90 per cent of patients who can tolerate this treatment. Lymecycline is usually the first-line systemic treatment as doxycycline occasionally causes photosensitivity or oesophagitis. Tetracyclines should not be used in children under the age of 12 years.
Acne is a chronic disease
Acne should be considered a chronic disease. Like many other chronic diseases such as asthma or rheumatoid arthritis, treatment should be aimed at settling the acute symptoms (papules, pustules, nodules and cysts) and preventing relapse. Once the patient’s acne is under control (90 per cent or clearer) they can stop their oral therapy, but should continue with their topical retinoids or retinoid-like agent indefinitely to prevent relapse until such time as they are convinced that they have grown out of their acne. This can be months or years if necessary.
Oral tetracyclines and topical retinoids or retinoid-like agents should be avoided in pregnancy. BPO and erythromycin 500mg twice a day for three-to-six months are safe in pregnancy if required for troublesome acne.
Adapalene (a topical retinoid-like agent) combined with BPO (Epiduo Gel) is a very useful product as it can be used both to control acute flare ups of acne (with a course of oral antibiotics for three-to-six months if necessary), and it can also be used as a maintenance treatment once the acne is under control to prevent relapse. With these combinations it may be possible to explain to the patient how to manage the acute phase of their moderately-severe acne (eg, Epiduo Gel and an oral anti-acne tablet for three-to-six months) and the maintenance treatment (eg, stop the tablet and use Epiduo Gel alone) in one single visit.
Lifestyle, cosmetics, and medication
Acne is primarily hormonally driven. However, poor diet, inappropriate use of cosmetics, stress and picking can all aggravate acne. There is some evidence that excessive sugar and excessive dairy in the diet may aggravate acne. When seeing a young person with acne it is a good opportunity to give them lifestyle advice about diet and exercise. Try to talk directly to the young teenager who comes with their parents. Encourage them to stay on a low-sugar diet and they should be encouraged not to consume excessive dairy products. Protein powders that are used for sports or bodybuilding should be avoided as they contain excessive amounts of whey protein and often make acne worse. While there is no hard evidence that exercise helps acne, it is a good opportunity to advise young people to take vigorous physical exercise for one hour at least five times a week, which may help their overall health and feeling of wellness.
| INDICATIONS FOR ORAL ISOTRETINOIN (ROACCUTANE) |
| – Severe nodulocystic acne – Acne unresponsive to standard oral and topical treatments especially if scarring – Acne relapsing after repeated courses of oral and topical acne therapies – Acne associated with severe psychological upset – Gram-negative folliculitis – Conglobate acne – Acne fulminans – Pyoderma faciale |
Young women in particular are bombarded with misinformation about skin care and cosmetics. They are encouraged to “cleanse, tone and moisturise”
even if they don’t need it. Moisturising already oily, acne-prone skin is like “adding fuel to the fire”. Young people should be informed that moisturising does not prevent wrinkles or ageing of the skin. However, some acne cleansers and topical acne treatments may dry the skin, so some patients may need a light-weight, oil-free, non-comedogenic moisturiser in the mornings to control the drying effects of their acne treatments. Make up and sun blocks should be oil-free and non-comedogenic.
Underlying hormonal issues, such as women using ultra-low-dose oestrogen combined contraceptive pills, progesterone-only pills, progesterone implants, or progestogen-containing intrauterine devices (IUDs) (eg, Mirena or Kyleena) may aggravate acne. Women with resistant acne or acne with signs of other hormonal problems such as irregular periods, obesity or hirsutism should be investigated for PCOS. Women with PCOS and acne may do well with hormonal treatments such as the contraceptive pill Dianette for up to 12 months or spironolactone (a diuretic that has been used off-label in women with acne for over 30 years due to its anti-androgenic properties) (50- 100mg daily), which can reduce oil production and comedones. These hormonal treatments are best combined with topical anti-inflammatory agents such as BPO or azelaic acid. Women on spironolactone should not become pregnant, due to potential risk of birth defects.
Patients with severe nodulocystic acne, scarring acne, and acne that does not respond or relapses as quickly to six months of an oral anti-acne agent combined with appropriate topical agents as outlined above may need a course of oral isotretinoin (Table 4). This should only be prescribed by doctors with experience of prescribing systemic retinoids (eg, GPs with a special interest in dermatology or consultant dermatologists).
References on request











Leave a Reply
You must be logged in to post a comment.