







Prof Brendan Kelly outlines approaches to help prevent deliberate self-harm and suicide
The rate of suicide in Ireland has been in decline for several years, but deliberate self-harm and suicide still remain real and urgent problems. Globally, over 800,000 people die due to suicide every year, and for every suicide there are many more people who engage in deliberate self-harm. Suicide is the second leading cause of death among 15 to 29-year-olds around the world.
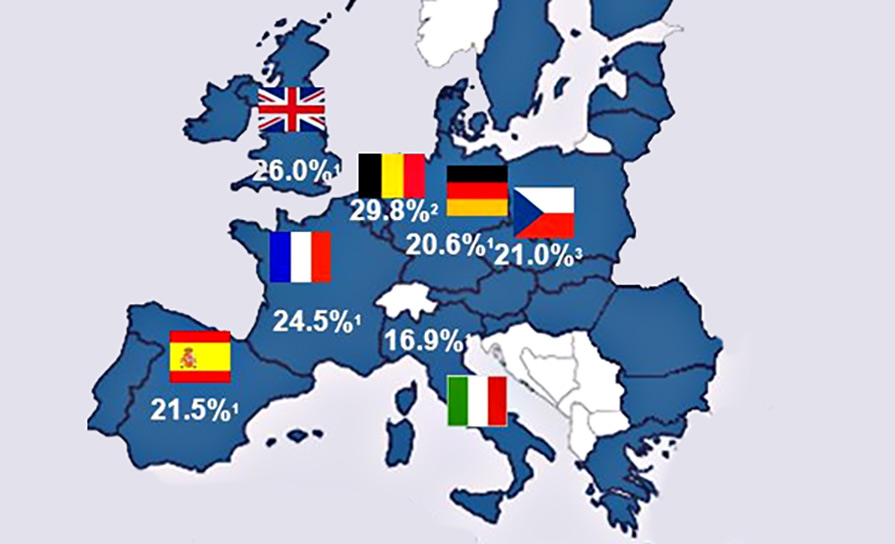
Rates of deliberate self-harm and suicide change significantly over time. In broad terms, recent years have seen a reduction in the rate of suicide in Ireland, despite the economic recession of 2008-13. But rates of deliberate self-harm and suicide are not evenly distributed across age groups and there are particular reasons to be concerned about younger adults, as rates of youth suicide are persistently very high in Ireland compared to other EU countries.
Risk factors for suicide and deliberate self-harm
Given the prevalence of suicide and deliberate self-harm, there have been extensive efforts to build models to try to predict deliberate self-harm and suicide and so provide better care. Key risk factors for non-fatal deliberate self-harm include female gender, younger age, poor social support, major life events, poverty, being unemployed, being divorced, mental illness and previous deliberate self-harm.
Key risk factors for suicide include male gender, poor social support, major life events, chronic painful illness, family history of suicide, mental illness and previous deliberate self-harm. For both deliberate self-harm and suicide, availability of means is also significant (eg, easy availability of tablets to take overdoses).
In terms of mental illness, suicide is associated with major depression (long-term risk of suicide: 10-15 per cent), bipolar affective disorder (10-20 per cent), schizophrenia (10 per cent) and alcohol dependence syndrome (15 per cent). In addition, individuals who engage in deliberate self-harm have a 30-fold increased risk of completed suicide over the following four years.
Despite these associations from the research, however, the majority of people with these risk factors will not die by suicide, because the increases in risk associated with these risk factors are small and, despite its tragedy and implications, suicide is (from a mathematical viewpoint) a statistically rare event, with fewer than 500 suicides per year in Ireland’s population of 4.7 million. As a result, it is statistically impossible to predict suicide at the level of the individual. This is true even for people who have thoughts of suicide, as the proportion of people with suicidal thoughts who go on to actually complete suicide is less than one-in-200. This suggests that simple population screening for suicidal thoughts is unlikely to be either effective or efficient in identifying individuals at risk of suicide.
Overall, then, it is impossible to predict suicide in any individual case. It is often the case that bereaved families believe that there were signs that they missed or that health professionals should have predicted the outcome in cases of suicide. Statistically, however, there is no way that anyone can predict suicide in an individual case.
Preventing suicide and deliberate self-harm
So, if it is impossible to predict suicide accurately at individual level, what can be done? Plenty can be done. Prompt and proper treatment of mental illness in primary and secondary care is central to reducing risk of suicide and self-harm.
In addition, and despite the impossibility of statistical or actuarial prediction in individual cases, careful, realistic exploration of risk factors is also very useful for guiding treatment and providing support to people who present with suicidal crisis or mental illness – although it must be remembered that these assessments do not provide a basis for statistical or actuarial prediction of precisely which individuals will engage in deliberate self-harm or suicide and which individuals will not.
As a result, even following careful psychiatric clinical evaluation, risk assessment, full treatment, risk management, communication with family and/or others (possibly necessitating breach of confidentiality in certain circumstances), and meticulous follow-up, it is still entirely possible that any given individual will engage in deliberate self-harm or suicide. All of the assessments, risk management and treatment services should, of course, be provided as appropriate to each individual case and they might well reduce risk in a general sense. But, even so, the outcome cannot be predicted in any given case: even with the very highest standard of assessment and care on any given day, deliberate self-harm or suicide can still occur on that same day and cannot be predicted.
In an overall sense, however, good mental healthcare, good communication with families, and good follow-up quite possibly might all help reduce general risk of suicide. In 2010, the College of Psychiatry of Ireland (as it was then called) noted that “effective treatment of depression is an important means of reducing suicide rates” and addressed the much-discussed role of antidepressant medication in adults in some detail.
Untreated depression can have a fatal outcome. Those experiencing moderate to severe depression frequently describe having thoughts of self-harm. Antidepressants are effective in the treatment of depression. The effective treatment of depression is an important means of reducing suicide rates. A huge volume of research in recent years has failed to establish a causal link between antidepressant use and suicide. At an individual level, the period early in treatment may be a time of relatively high-risk, as treatment tends to start when the person’s depression is severe and takes some weeks to work. As treatment takes effect and energy and motivation return, people who have recently commenced antidepressant treatment may be more able to act on suicidal thoughts that are inherent to their condition. That the early recovery period is potentially a period of increased risk for suicidality is something of which all doctors should be aware. The College of Psychiatry of Ireland, in unison with the advice of the Irish Medicines Board, recommends close monitoring of all individuals commenced on antidepressant therapy. There is no evidence of a link between antidepressant use and homicide (College of Psychiatry of Ireland, Antidepressant Medication – Clarification. Dublin: College of Psychiatry of Ireland, 2010).
Good treatment of depression in primary care is essential in trying to reduce suicide rates, as is treatment of substance abuse, including alcohol misuse. Other specific mental disorders should also be treated in their own ways; eg, use of lithium in bipolar disorder (manic depression) might help reduce suicide in this group. In emotionally unstable personality disorder, psychological therapies can prove very helpful, including adaptations of cognitive-behaviour therapy (CBT) and dialectical-behaviour therapy (DBT). DBT is somewhat similar to CBT and also involves group sessions, building skills such as mindfulness, and developing coping strategies other than deliberate self-harm for dealing with emotional instability. DBT is a challenging therapy but it can be highly effective for reducing self-harm in certain conditions, including (but not limited to) emotionally unstable personality disorder.
What should I do if someone says they are suicidal?
If someone tells you that they are suicidal, it is incredibly important that you take them seriously and take the time to listen to them. Doing this is more important than whatever you were doing just before the person told you how they are feeling (no matter what that was). You need to settle down and take some time with this.
At all times, listening and devoting time to people who are depressed or suicidal is absolutely vital. Remain calm and collected. If you think someone might be suicidal, but you are not certain, asking them directly does not increase risk. It does not ‘put the idea into their head’. For example, if a person says they are feeling very depressed and hopeless about the future, you can ask: “Are there times when you feel so low that you feel like you can’t carry on? That you want to end your life, or kill yourself?”
Contrary to what many people think, asking in this direct fashion does not increase risk. Nor does asking the person to tell you more about how they are feeling, if they are hesitant or unclear. Most people are hugely relieved to talk about their distressing thoughts with someone who has the capacity to listen and not be overwhelmed by what is said. Someone who will actively listen, really hear what they say, and demonstrate that they care.
Language matters greatly. Mostly listen. When you speak, avoid platitudes. For example, do not say: “Don’t worry; everything is okay.” Clearly, everything is not okay. Saying that everything is okay just confirms the person’s worst fear – that you are not really hearing them. As they see it, everything is most certainly not okay. It is also generally not helpful to tell people that things could be worse. You do not know if that is true, and, even if it is, the person probably thinks things cannot possibly get any worse. That is why they feel the way they feel. It might not be true, but it is how they feel right now.
And you are not there to argue with them. For now, you are there just to be there. And that might well be enough for the moment. Listening is the most important thing you can do. You can challenge some of their interpretations or beliefs some other day, when matters are less acute.
For now, simply listen. Take your time. Ignore your phone. Do not feel the need to speak every time there is a silence. The most important thing that you are doing is being there.
After a while, make one or two very pragmatic, very short-term suggestions; eg, “Let’s go for a walk while you tell me more about this.” At the outset, avoid making more long-term suggestions, eg, “Maybe you should quit your job” or “Why not leave your husband?” These are issues for another day. Be generally hopeful, but remember that simplistic solutions to long-term problems can seem trite and unrealistic. Just focus on today. Do not panic or let yourself get overwhelmed. Do not blame the person. Remain calm, pragmatic and hopeful as you speak and make a plan of action.
When making a plan of action, there is good advice on the website of SpunOut.ie about what to do when someone is feeling suicidal. In the first instance, if the person has already taken steps to end their own life it is important to call 999 immediately to get them medical attention, or take them straight to an emergency department in a hospital.
If they have not already taken steps to end their life, but remain suicidal, it is useful to stay with the person and remove means of self-harm from their immediate vicinity (eg, tablets). It is also useful to assist the person in accessing one of the support services available, depending on the situation.
The Samaritans (www.samaritans.org) provide a listening service to anyone who contacts them, many of whom are contemplating suicide (telephone 116 123; email jo@samaritans.org). Pieta House (www.pieta.ie) also offers support for anyone who is suicidal (telephone 1800 247 247). Other sources of support include GPs and community mental health teams.
In the more acute situation, most large and regional hospitals have psychiatry services operating 24 hours a day, seven days a week, 365 days a year. Where the local inpatient unit is located within a general hospital, emergency and out-of-hours psychiatry assessments generally occur in the emergency department of the hospital. This is often a difficult setting for such assessments to occur, but staff try to make the circumstances as therapeutic as possible. For inpatient units that are not located in general hospitals (eg, stand-alone psychiatric hospitals), emergency assessments sometimes occur in the hospital itself or in a neighbouring general hospital.
It is important at all times to remain calm and supportive, and really listen to what is being said. By confiding in you, the person has placed you in a very privileged and very responsible position. And remember, while this might be the first time you have had a conversation like this, thoughts of self-harm and suicide are, regrettably, far more common than most people imagine.
Public health measures
From a public health perspective, public education and measures to limit access to means of self-harm are very important and effective in reducing suicide and suicidal behaviour. Regulations governing paracetamol sales are an excellent example as they greatly reduce harm resulting from paracetamol overdose in Ireland and elsewhere. Placing barriers at known suicide locations (eg, certain bridges) is another very effective method for deterring self-harm and suicide. Research shows that a great number of people who are deterred or delayed in this fashion will re-consider their suicidal thoughts and very many will not proceed to find other means of self-harm.
Good primary care, good mental healthcare, and appropriate public health measures, are, then, essential for addressing the problems of deliberate self-harm and suicide at national level in Ireland. These measures should be aimed at everyone, not just those with thoughts of deliberate self-harm or suicide. Often, there are no warning signs.
In 2015, a new suicide prevention strategy was launched by Healthy Ireland, the Department of Health, HSE and the National Office for Suicide Prevention, titled Connecting for Life: Ireland’s National Strategy to Reduce Suicide, 2015-2020. The strategy involves preventive and awareness-raising work with the population as a whole, supportive work with local communities, and targeted approaches for priority groups. The strategy proposes high-quality standards of practice across service delivery areas and – most importantly – an underpinning evaluation and research framework.
Approaches rooted outside of core mental health services will be vital in this process: Addressing alcohol problems and other addictions, reducing homelessness, reforming the criminal justice system, and improving access to social care.
This matters to everyone. Everyone knows a family affected by suicide. Grief following suicide is especially complex and difficult. Families often experience shock, loss, guilt, shame, anger, and many other emotions. They may not feel able to identify with families who are bereaved in other ways. They may feel isolated and that there is a lack of understanding.
Those who are bereaved by suicide are by no means alone, but it can be difficult to reach out to others. Support groups can prove very helpful, as can discussions with members of the primary care or mental health teams. Pieta House also offers support, both for those bereaved and those who are feeling suicidal.
Useful resources
Individuals with any mental disorder or psychological problem, and their families, will find much that is useful on the Internet. As ever, Internet resources need to be evaluated with care and only trusted when the information comes from a reliable source. Reliable information about mental health can be sourced from the websites of the HSE (www.hse.ie/eng/health/az), College of Psychiatrists of Ireland (www.irishpsychiatry.ie), Royal College of Psychiatrists in London (www.rcpsych.ac.uk), National Health Service in the UK (www.nhs.uk) and National Institute of Mental Health in the US (www.nimh.nih.gov).
Evidence-based guidance about specific treatments can be found on the website of the UK National Institute for Health and Care Excellence (NICE) (www.nice.org.uk).
Information about suicide around the world is available from the World Health Organisation (www.who.int/topics/suicide/en) and there is further information available from Ireland’s National Suicide Research Foundation (www.nsrf.ie) and National Office for Suicide Prevention (www.nosp.ie).
In addition to the above, there are several books which may also be helpful, including:
The Savage God: A Study of Suicide by Al Alvarez (Weidenfeld and Nicolson, 1971).
A Concise Guide to Understanding Suicide: Epidemiology, Pathophysiology, and Prevention edited by Stephen H Koslow, Pedro Ruiz and Charles B Nemeroff (Cambridge University Press, 2014).
The International Handbook of Suicide Prevention (Second Edition) edited by Rory C O’Connor and Jane Pirkis (John Wiley and Sons Ltd, 2016).










Leave a Reply
You must be logged in to post a comment.