NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Cystic fibrosis and lung transplantation in the era of CFTR modulators
By
Dr Suzanne Carter
- 05th Mar 2023
Cystic fibrosis (CF) is an autosomal recessive disorder caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. CF is a life-limiting condition with multi-system involvement characterised predominantly by respiratory and extra-pulmonary manifestations including disease of the pancreas, liver, and gastrointestinal tract. In 2020 there were 1,466 people with CF receiving care in Ireland.
In recent years, survival rates in CF have improved significantly with a median predicted survival for those born between 2016 and 2020 of 50 years. This is reflective of focused therapies and better understanding of the management of multi-system manifestations. The recent development of highly-effective modulator therapies (such as ivacaftor and elexacaftor-tezacaftor-ivacaftor) has led to improved outcomes for people with CF and removal of some people with CF from transplant waiting lists.
However, the increasing complexity of care for an older CF population may present new challenges such as renal failure, drug-resistant organisms, or co-morbidities of later life, which may impact on suitability for transplant.
For patients with advanced lung disease, lung transplant remains a key therapeutic option with potential to improve quality-of-life and extend life expectancy. According to the International Society for Heart and Lung Transplantation (ISHLT), CF represents the third most common indication for lung transplant.
Advanced CF lung disease is a key indicator for consideration for transplant referral, and is defined as forced expiratory volume in one second (FEV1) of less than 40 per cent predicted value. Other criteria that may prompt referral for transplant evaluation include hypercapnia (pCO2 >6.6kPA on arterial blood gas testing), previous ICU admission for respiratory failure, day-time oxygen requirement, pulmonary hypertension (pulmonary artery systolic pressure of >50mmHg on ECHO) or a six-minute walk test (6MWT) of less than 400 metres.Other comorbid factors such as CF-related diabetes, rapidly declining FEV1, exertional oxygen requirement, and the number of pulmonary exacerbations are significant in identifying patients who may deteriorate more rapidly.
Currently, it is estimated that the median survival post-lung transplant is on average 6.7 years. Lung transplantation survival secondary to CF is associated with a median survival of 9.9 years, increasing to 12.4 years for those who survive the first year. Lung transplant is a life-prolonging procedure, which carries significant risk and every case is unique and individualised. Early referral and identification of appropriate patients is important for early optimisation of co-morbidities, allowing the patient the opportunity to address the modifiable barriers and to minimise post-operative complications.
Pre-operatively
CF is a multi-organ disease and optimisation of co-morbidities is essential in the lead-up to transplant. Factors such as extremes of body mass index (BMI), poorly controlled diabetes, renal impairment, and oesophageal dysmotility are associated with higher rates of complications and poorer outcomes after transplant. Compliance, substance misuse and other psychosocial factors must also be taken into account.
Incidence of gastro-oesophageal reflux disease (GORD) increases significantly in the post-transplant period, with untreated disease contributing to pulmonary infection and deterioration in lung function. People with CF (PWCF) are pre-disposed to GORD, with 55 per cent of Irish adult CF patients reporting significant symptoms. Optimisation of medical management and consideration for surgical intervention should be addressed early to reduce symptomatic burden post-operatively.
Low BMI is an independent risk factor for mortality in PWCF. A BMI of less than 18 is associated with a higher risk of mortality in the first year following transplant. While referral for transplant should not be delayed for this alone, optimisation of nutritional status should be addressed prior to formal assessment.
CF treatment is complex and carries significant burden over prolonged periods of time. Poor compliance to therapies is associated with higher exacerbation rates. Adherence to prescribed medications appears to be better than to physiotherapy regimens or nutritional supplements. Evidence of poor compliance in the pre-transplant setting must be considered in the work-up for lung transplant, along with other psychosocial factors, as a possible indication of poor adherence in the post-transplant setting.
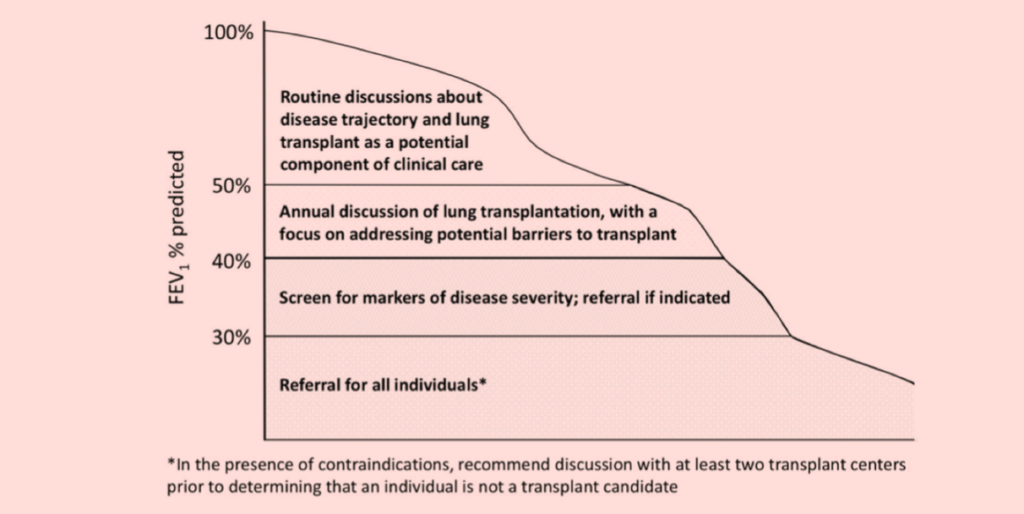
Figure 1
Consensus guidelines to identify patients who would benefit from lung transplant consideration referral were published by the Cystic Fibrosis Foundation in 2019. The goal of this document was to help clinicians to identify any potential barriers to transplant earlier than traditional referral models in order to achieve successful outcomes. It recommends the early referral of appropriate patients to avoid the need for emergent transplant (Figure 1). It focuses on early communication with patients and their families to enhance the referral process.
Peri-operatively
Double lung transplant is recommended in PWCF due to the risk of cross-contamination and infection associated with a single lung transplant. Chronic bacterial colonisation and multi-drug resistant organisms are common in CF, resulting in complex antimicrobial management in the peri-operative period. In addition to routine local practice for peri-transplant antibiotics, intraoperative specimens and previous cultures need to be taken into account when devising appropriate targeted antimicrobial regimens. Three-monthly screening for bacterial, fungal and mycobacterial pathogens for people with CF on the active transplant list is advised.
Infection with Burkholderia cenocepacia complex (BCC) or Mycobacterium abscessus are considered contraindications to transplant due to increased risk of post-transplant mortality.
Annual incidence of pneumothorax in CF is 0.64 per cent and is more common in those of older age with advancing pulmonary disease. While not a definite contraindication to transplant, special consideration needs to be given to these patients peri-operatively. There is an increased associated risk of bleeding in those who have had previous thoracic procedures such as pleurodesis, but no evidence of increased mortality.
In some centres worldwide, ECMO (extracorporeal membrane oxygenation) has been used as a bridge to transplant. ECMO is associated with increased complication rates and is only available in specialist centres.
In recent years, survival rates in CF have improved significantly with a median predicted survival for those born between 2016 and 2020 of 50 years
Post-operatively
The Cystic Fibrosis Foundation highlights the importance of multidisciplinary CF care to ensure follow-up and treatment for extra-pulmonary complications of CF within six-to-12 months of lung transplant.CF sinus disease is often implicated in respiratory deterioration and infection post-transplant. Specialist assessment and endoscopic surgery can be beneficial for symptomatic patients. It has been shown that there is some relationship between pre-transplant sinus cultures and post-transplant bronchoalveolar lavage cultures, which suggests that sinuses remain a reservoir for post-transplant allograft infection. Antibiotic prophylaxis and airway clearance techniques are important to consider post-transplant. As there is insufficient evidence for DN-ase, hypertonic saline, and airway clearance post-transplant, individualised decision-making regarding management, and continuation of inhaled antibiotics should be considered.
Liver enzymes should be monitored at a minimum annually, with imaging as appropriate, noting the additional potential for drug hepatotoxicity post-transplant. Altered pharmacokinetics result in a need for increased vigilance in monitoring immunosuppressant levels in the CF population.
Screening for diabetes with OGTT should take place three-to-six months post-transplant in those without pre-existing CF-related diabetes and annually thereafter.
Given the risk of osteoporosis and CF-related reduced bone mineral density, a DXA scan should be scheduled for six-to-12 months post-transplant.
Renal dysfunction can be present pre-transplant in CF and is often multi-factorial (diabetes, aminoglycosides, nephrolithiasis and infections). Abnormal renal function is common in CF lung transplant recipients, requiring close monitoring of immunosuppressant levels and referral to nephrology. At two years, 35 per cent of CF lung transplant recipients will have post-transplant renal dysfunction.
Pregnancy is not advised for the first two years post-transplant due to increased risk of acute and chronic rejection and death, and beyond two years it is only suitable in a small subgroup of patients and carries significant risk.
Overall risk of cancer increases post-transplant by a factor of 2.7 in non-CF recipients and 10-fold in CF lung transplant recipients compared to the general population. The risk of colorectal cancer increases to 25-to-30-fold in CF lung transplant recipients compared to the general population.Colorectal cancer screening should commence at the age of 40 years in all people with CF and rescreening should occur at three-to-five years depending on initial results.
Dietetic input is required post-transplant to ensure adequate levels of fat-soluble vitamins, optimisation of BMI, and glycaemic control.
Conclusion/future
Lung transplant recipients with CF have complex care needs crossing many specialties. Dedicated clinics with specialist input are important to address both post-transplant requirements, but also the unique CF-related co-morbidities, which continue to contribute significantly to patient morbidity post-transplant.
Multi-organ transplants have been carried out either simultaneously (lung and liver, lung and pancreas, and lung-liver-pancreas) or staged (lung, liver, pancreas, kidney) in CF with varying success rates.Factors impacting on the feasibility and safety of simultaneous transplants include operative risk, expertise and wait times in the context of multi-organ allocation.
The introduction of CFTR modulators has revolutionised care in CF. Initial trials assessing the efficacy of these modulators in the CF population excluded patients with advanced pulmonary disease. However, clinical experience has seen patients defer listing for transplant as a result of positive outcomes from modulator treatment. While large-scale studies to examine the effect of CFTR modulators on extra-pulmonary manifestations in the post-transplant setting are yet to be carried out, a recent study has reported outcomes for 94 patients prescribed elexacaftor-tezacaftor-ivacaftor post lung transplant. Improvements in HbA1c and anaemia were observed with no effect on BMI noted. Only 3 per cent developed elevated liver enzymes, but 42 per cent stopped treatment due to side-effects and lack of perceived benefit.
Lung transplantation can improve survival and quality-of-life in people with CF and advanced lung disease. With advances in CF modulators and improvements in outcomes, the role of early discussion and referral has become more important in the setting of an older, potentially more complex, population. Early referral and discussion of transplant allows opportunities to overcome any potential barriers to transplantation and ensure optimal timing and outcomes from transplantation.












Leave a Reply
You must be logged in to post a comment.