NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Crohn’s disease (CD) is a chronic idiopathic inflammatory bowel disease (IBD) with a complex aetiology involving genetic, environmental, and immunological factors. It is characterised by recurring episodes of inflammation, ulcerations, and strictures, leading to a wide range of symptoms and complications.1
Over 40,000 people in Ireland are living with IBD. Of these, approximately 20,000 are affected by colitis and CD.6 CD can affect people of any age, but usually starts between the ages of 15 and 35, while a second, smaller peak can occur from the ages of 50-to-70. CD affects men and women equally, with a slight female predominance in adult-onset. Incidence and prevalence are higher in high-income countries and in urban areas, with a notably large incidence in Northern Europeans and among the Ashkenazi Jewish population.1,4 IBD is complex and costly, and its increasing prevalence places a greater stress on healthcare systems.9
CD can affect any part of the gastrointestinal tract. Fifty per cent of patients have terminal ileum and colon involvement, while 30 per cent have small bowel-only involvement, and 20 per cent of cases are isolated to the colon. In addition, 25 per cent of patients experience perianal complications, including fissures and fistula. Less frequently, patients present with isolated perianal complaints, upper gastrointestinal disease, or extra intestinal manifestations (EIMs), which can affect the skin, joints, eyes, liver, blood vessels, and kidneys. Arthritis is the most common EIM, affecting up to 25 per cent of patients with CD. There is no cure and most patients experience bouts of remissions and relapse at unpredictable times.1
In CD, the inflammation extends through the entire thickness of the bowel wall from the mucosa to the serosa. The disease runs a relapsing and remitting course. With multiple relapses, it can progress from an initially mild or moderate inflammatory condition, to a severe penetrating and stricturing disease. CD has a significant impact on the quality-of-life of affected individuals, necessitating early diagnosis and appropriate management strategies.1
Image 1
Pathophysiology
The pathophysiology of CD is multifactorial in nature, involving genetic predisposition, infectious, immunological, environmental, and dietary factors. A major role is played by alterations at the level of immunity and inflammation. Innate immunity is involved in terms of defects in the mucous barrier (MUT2 and FUT2 genes), while adaptive immunity relies on a TH1 lymphocytic response and TREG cells mediated by cytokines, like tumour necrosis factor (TNF)-α, IL-12, IL-34, and IL-23. The increased migration to the sites of inflammation is also determined by a reshaping of the extracellular matrix through the action of metalloproteins MMP-1 and MMP-3, and the over-expression of adhesion molecules such as MAcCAM-1 and integrin α4β4.2
The characteristic transmural inflammation can include the entire gastrointestinal (GI) tract from mouth to the perianal area; although it most frequently involves the terminal ileum and right colon. The initial lesion starts out as an infiltrate around an intestinal crypt. This leads on to ulceration, first in the superficial mucosa, and then the deeper layers. As the inflammation progresses, non-caseating granulomas form that involve all layers of the intestinal wall. It can develop into the classic cobblestone mucosal appearances and skip lesions along the length of the intestine, sparing areas with normal mucosa. As the flare of CD settles, scarring replaces the inflamed areas of the intestines. Granuloma formation is very common in CD, but absence does not exclude the diagnosis. Ongoing inflammation and scarring can lead to bowel obstruction and stricture formation. CD is also associated with enterovesical, enteroenteral, enterocutaneous, and enterovaginal fistulas.3,4
Risk factors
Environmental factors can include smoking, antibiotics, non-steroidal anti-inflammatory drugs, and reduced fibre diet. While the role these factors play is not fully known, they can act as triggers to initiate a harmful immune response in the GI tract.8 Smoking is the most notable risk factor for developing CD, aside from family history and ethnic background. Smokers are twice as likely as non-smokers to develop the condition, and those who smoke usually experience more severe symptoms compared to those with the condition who do not smoke. While there is no evidence that diet plays a role in CD, certain types of food and drink have been associated with worsening symptoms, including milk, dairy products, alcohol, processed, spicy, and fatty foods. There is no diet or eating plan that will work for everyone with CD, and dietary recommendations must be tailored individually. Some research suggests that a Mediterranean style diet is associated with an improved quality-of-life and reduced disease activity. Some probiotics have also demonstrated small benefits. Although flares are often associated with stressful events, there is no evidence to prove that stress causes or contributes to the disease.1,6,7
Presenting symptoms
There are three main phenotypes of CD – inflammatory, stricturing, and penetrating. Presenting symptoms are variable and some patients may have symptoms for years before a diagnosis of CD is made. Patients with inflammatory disease often present with abdominal pain and diarrhoea, and may develop more systemic symptoms like weight loss, low-grade fevers, and fatigue. Patients with stricturing disease may develop bowel obstructions, while those with penetrating CD can develop fistula or abscesses. When an abscess is present, in addition to abdominal pain, patients can have systemic symptoms such as fever and chills, and may also present with signs of acute peritonitis.5
Diagnosis
The diagnosis of CD can be quite challenging given that presenting symptoms can be insidious and nonspecific. A detailed patient medical history and physical examination is essential. Blood tests can highlight the presence of anaemia (B12 or iron deficiency) or liver disease. Special serology, such as normal anti-neutrophil cytoplasmic antibodies (ANCA) and raised anti-saccharomyces cerevisiae antibodies (ASCA), can distinguish CD from ulcerative colitis. C-reactive protein (CRP) or erythrocyte sedimentary rate (ESR) can reflect the severity of the inflammation. Stool tests to rule out infections include culture and sensitivities, ovum and parasites, clostridium difficile toxins, and leukocyte count. Stools for calprotectin can detect active CD. Plain x-rays are ordered if bowel obstruction is suspected. The perineum should be examined in all patients, and may reveal skin tags, ulcers, fistulas, scarring, and abscess. Frank perforation is rare, but can be a presentation of CD.1
Symptoms that require further investigation include weight loss, bloody diarrhoea, iron deficiency, and night-time awakenings. A significant family history of IBD, unexplained elevations in CRP, ESR, or other acute phase reactants like ferritin, platelets, or low B12 should prompt further investigation.1
There is no single test that can be used to confirm or disprove a diagnosis of CD. The diagnosis is made based on symptoms and diagnostics that may include:
Colonoscopy;
Biopsy;
Small bowel enteroclysis (SBE);
CT and/or MRI;
Wireless capsule endoscopy.
Pathology can also be confirmatory of CD.1,5,7 Endoscopy with histological evaluation remains the gold standard for diagnosing CD. However, advanced imaging techniques, such as magnetic resonance enterography (MRE) and computed tomography enterography (CTE), have emerged as valuable tools for evaluating disease extent and complications. Biomarkers, such as faecal calprotectin and CRP, aid in disease monitoring and predicting disease activity.1,5
Complications
CD is associated with extraintestinal manifestations including episcleritis, uveitis, stomatitis, aphthous ulcers, liver steatosis, gallstones, cholangitis, primary sclerosing cholangitis, nephrolithiasis, hydronephrosis, urinary tract infections, arthritis (sacral spine, knee, ankles, hips, wrist, elbows), ankylosing spondylitis, erythema nodosum, and pyoderma gangrenosum. Thromboembolic disease can also be a complication, and may present as deep vein thrombosis, stroke, or pulmonary embolism. Patients with CD also have an increased risk of developing colorectal cancer.1,4
Differential
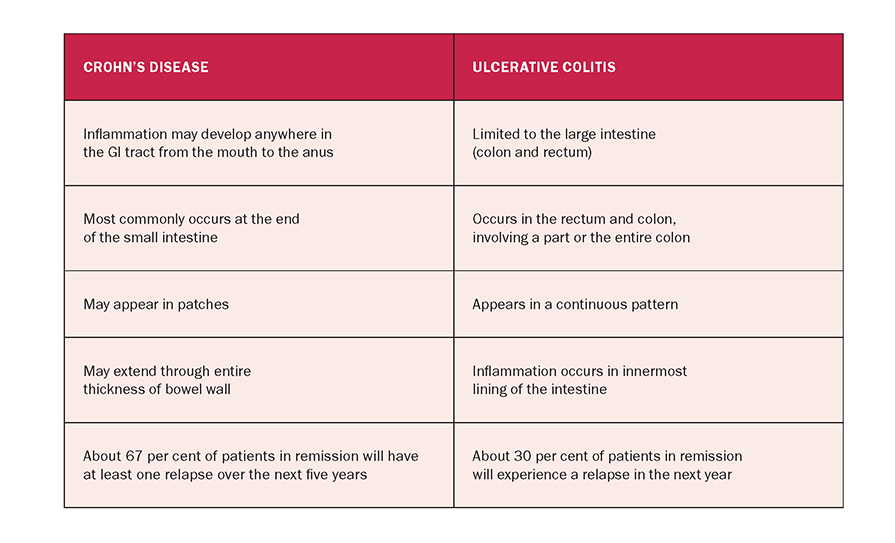
Other conditions can mimic the symptoms of CD and it is important to rule out infection and other causes, even when patients with known CD are having flare-ups. Patients with diarrhoea should be assessed for infection, inflammation, and in certain cases, coeliac disease. Other conditions that may present like CD include appendicitis, Behcet’s disease, and ulcerative colitis.1 It is important not to confuse IBD with irritable bowel syndrome (IBS). IBS is a disorder that affects the muscle contractions of the bowel and is not characterised by intestinal inflammation, nor is it a chronic disease.8 CD and colitis are both inflammatory diseases, but there are some notable key differences that are outlined in Table 1.8
Treatment and management
The diagnosis, treatment, and management of CD requires a multi-professional approach. Patient education regarding the illness is a vital component of management. There are several medications available to treat CD, however, there is no cure. The mainstay of treatment is medical therapy, with the goal of achieving clinical, endoscopic, and histologic remission, demonstrated by mucosal healing. Treatment is chosen based on the disease stage, severity, and location. Dietician input and nutritional supplementation are highly recommended before and during the treatment of CD.1,4
Steroids
Steroids are used to induce remission, but are not an effective maintenance agent. Steroids are usually only used to treat the active disease because their long-term use is associated with a range of adverse side-effects. Budesonide and prednisolone are the two varieties most commonly prescribed.1,5,7
Budesonide is usually the first choice of steroid prescribed to help control the symptoms of CD. Taken on a short-term basis of less than 12 weeks, budesonide may cause acne, oedema of the face, hands, arms, feet and legs, mood changes, insomnia, and indigestion. If taken for more than 12 weeks, budesonide may cause osteoporosis, increased vulnerability to infection, cataracts, muscle cramps, and stiffness. Vitamin D and calcium supplements may be required to help protect against the effects of osteoporosis. Due to increased vulnerability to infections, close contact with people who are known to have infections, particularly those with chickenpox, measles, and shingles should be avoided.1,5,7
Prednisolone is used in cases where budesonide proves ineffective. It has the same type of short- and long-term side-effects as budesonide, and has also been known to cause mental health problems in an estimated 5 per cent of people.1,5
Table 1: Key differences between CD and ulcerative colitis
Aminosalicylates
Sulfasalazine belongs to a group of medicines called aminosalicylates, used to reduce inflammation inside the colon. Sulfasalazine can be used as an alternative to steroids to treat mild cases of CD. Common side-effects include headache, nausea, abdominal pain, and diarrhoea.1,5
Immunosuppressants
Immunosuppressants are used in maintenance therapy and in combination with steroids when a person has a relapse of symptoms. Immunosuppressants used for treating CD include methotrexate, azathioprine, tacrolimus, and mercaptopurine. Side-effects of azathioprine include increased vulnerability to infection, bleeding, and bruising. Less common side-effects include headaches, shortness of breath, dizziness, nausea, and vomiting.1,5,12
Mercaptopurine, originally developed to treat leukaemia, has since shown efficacy in the treatment of CD. Given in tablet form, its side-effects are not as severe as those associated with other forms of chemotherapy treatment. Common side-effects do include nausea and vomiting, while less common side-effects include loss of appetite, fatigue, breathlessness, and weakness caused by anaemia. Effective contraception if sexually active is also important taking mercaptopurine, as it temporarily affects both ova and sperm, and can increase the risk of birth defects.1,5
Biological therapies
Biological therapies are a modern medication created using naturally occurring biological substances such as antibodies and enzymes. Two main biological therapies are infliximab and adalimumab. Infliximab is usually only recommended in severe cases of disease that have not responded to steroid and immunosuppressant treatments, and where the person is unsuitable for surgery.1,12
Infliximab works by targeting the TNF antibodies that are responsible for much of the inflammation associated with CD. Given by intravenous infusion, around one-in-four people may have an allergic reaction to infliximab, with symptoms including joint and muscle pain, itchy skin, high temperature, rash, swelling of the hands and/or lips, problems swallowing, and headaches. Symptoms range from mild-to-severe and usually develop in the first two hours after the infusion has finished.1,5,11
Adalimumab works in a similar way to infliximab, by targeting TNF antibodies. It is given by injection and most people will need to have an injection every two weeks. Like infliximab, adalimumab increases vulnerability to infection, and those taking it should avoid contact with people with chickenpox or shingles, and always report any symptoms of a possible infection to the GP. Adalimumab can also cause reactivation of the hepatitis B virus and may not be suitable for people who were previously infected. Common side-effects of adalimumab include pain, swelling, redness, and itching at the site of the injection, headache, abdominal pain, nausea, vomiting, skin rash, muscle, joint and bone pain, and respiratory tract infections like colds and pneumonia.1,5,11
The goal of management is to control the inflammation and induce a clinical remission with pharmacological therapy, however, most patients will eventually require surgery. Surgery is not curative, and patients still require ongoing therapy even after surgery to prevent disease recurrence.1,6
Surgery
Surgery is required when the symptoms of CD cannot be controlled using medication alone, and for complications such as bowel obstructions, abscess, fistulas, or perforated bowel. During surgery, the inflamed section of the digestive system is removed and the remaining part is reattached. An estimated 80 per cent of people with CD require surgery at some point in their life. Surgery does not cure the disease, but it can provide long periods of remission, often lasting several years. A stoma may be required if the disease or inflammation is so severe that an immediate anastomosis is not safe. In some instances, the stoma may be temporary and can be closed once the severe inflammation and infection is controlled. A colostomy is also required if the rectum is removed.1,5,6,10
Despite optimal therapy, patients with CD often report an impaired quality-of-life, and life expectancy is slightly reduced due to the risk of development of malignancies, genitourinary disease, liver, and biliary tract complications. A holistic person-centred approach is required in the management of patients with CD, who face a lifelong challenging condition that can be emotionally and physically debilitating. The role of the healthcare professional is to provide ongoing assessment, management, support, and education. Key roles involve establishing a therapeutic relationship with the patient, assessing their understanding of the condition, establishing goals and expectations for successful management of their condition, and evaluating their physical, emotional, and psychological wellbeing.
Common concerns for patients are adherence to their therapeutic regimen, pain, and discomfort. Many patients experience anxiety, anger, frustration, stress, and depression, and their psychological needs should be adequately addressed. Assessment, monitoring, audit and evaluation for disease activity, progression, and the effects of the therapeutic regimen on a patient with CD is a continuous process. By implementing person-centered care, monitoring and evaluating symptoms, outcomes, and responses to therapy, clinicians play a pivotal role in managing the illness and improving the patient’s quality-of-life.
Complementary and alternative medicine
Some people report that complementary and alternative medicines (CAM) (including fish oils and probiotics) are helpful in controlling certain symptoms of CD, however, there is little scientific data to support their effectiveness. Although many types of CAM are generally safe, issues of purity, contamination with toxic metals, lacing with prescription drugs, and the side-effects of some traditional herbal remedies must be considered. Large well-designed randomised control trials are needed to validate specific CAM therapies before they can be incorporated into evidence-based medical treatments.13
Support groups
Crohn’s and Colitis Ireland (CCI) is a support organisation in Ireland for people who are living with, or impacted by, IBD. CCI work to improve the quality-of-life and wellbeing of the IBD community through sensitive support services, including advocacy, provision of information, training, and events. They also encourage and educate healthcare professionals in the importance and value of peer support as an adjunct to their management of IBD.l
Immunobiology: Impaired intestinal barrier function and dysregulation of the innate and adaptative immune system responses, with an alteration of gut microbiota
Deficient mucus biofilm barrier: Decreased expression of mucin secretion genes (MUC1, MUC19, and PTGER4) in the terminal ileum in patients with Crohn’s disease (CD)
Permeability changes in the intestinal epithelium: Altered expression of tight junction proteins (claudin)
Paneth cell dysfunction
Impaired autophagy of invasive microbes
Imbalance of effector T-cells and naturally regulatory T-cells
Recruitment and erratic retention of leukocytes
Dysbiosis:
Continuous alterations in intestinal microbiota resultin in clustering and reduced diversity in Firmicutes and Bacteroidetes phyla
Reduction in Faecalibacterium prausnnitzii was associated with an increased recurrence of ileal CD in the post-operative setting
Genetic risk factors:
Increased risk for individuals who have family history
Concordance in monozygotic twins is 20-to-50 per cent compared with 10 per cent in dizygotic twins
Wide genome association studies identified 200 loci associated to CD; however they contribute only a modest relative risk increase
NOD2, ATG16L1, IL23R gene variants are responsible for some of the heritable risk
Environmental risk factors:
Cigarette smoking doubles the risk of developing CD
Reduced fibre dietary intake
Antibiotic therapy during childhood increases the risk of developing CD
Other medications including non-steroidal anti-inflammatory drugs, oral contraceptives, and aspirin
Breastfeeding appears to be a protective factor against the development of CD
References
1. Ranasinghe IR, Hsu R. Crohn’s disease. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available at: www.ncbi.nlm.nih. gov/books/NBK436021/
2. Petagna L, Antonelli A, Ganini C, et al. Pathophysiology of Crohn’s disease inflammation and recurrence. Biol Direct. 2020;15(1):23. doi:10.1186/s13062-020-00280-5 3. Greuter T, Piller A, Fournier N, et al. Upper gastrointestinal tract involvement in Crohn’s disease: Frequency, risk factors, and disease course. J Crohns Colitis. 2018;12(12):1399- 1409. doi:10.1093/ecco-jcc/jjy121 4. Ricaurte Archila L, Hagen C. Colon inflammatory bowel disease. Crohn’s disease. 2022. Available at: www. pathologyoutlines.com/topic/coloncrohns.html 5. Feuerstein JD, Cheifetz AS. Crohn’s disease: Epidemiology, diagnosis, and management. Mayo Clinic Proceedings. 2017;92(7):1088-1103. Available at: http://dx.doi. org/10.1016/j.mayocp.2017.04.010 6. Crohn’s and Colitis Ireland. Supporting people living with, or impacted by Crohn’s disease or ulcerative colitis in Ireland. 2023. Available at: https://crohnscolitis.ie/ 7. Health Service Executive Crohn’s disease. 2021. Available at: www2.hse.ie/conditions/crohns-disease/ 8. AbbVie. Understanding Crohn’s and colitis. 2023. Available at: www.crohnsandcolitis.com/crohns/causes 9. Coward S, Clement F, Benchimol E, et al. Past and future burden of inflammatory bowel diseases based on modelling of population-based data. Gastroenterology. 2019;156(5):1345- 1353.e4. Available at: https://doi.org/10.1053/j. gastro.2019.01.002 10. Brown S, Fearnhead N, Clark S, Clifford S, et al. The Association of Coloproctology of Great Britain and Ireland consensus guidelines in surgery for inflammatory bowel disease. Colorectal Dis. 2018. Dec;20(8):3-117 11. Inokuchi T, Takahashi S, Hiraoka S, Toyokawa T, Takagi S, et al. Long-term outcomes of patients with Crohn’s disease who received infliximab or adalimumab as the first-line biologics. J Gastroenterol Hepatol. 2019. Aug;34(8):1329-1336 12. Brady E. An overview of Crohn’s disease. The Medical Independent. 2021. Available at: www.medicalindependent. ie/clinical-news/an-overview-of-crohns-disease/ 13. Lin S, Cheifetz A. The use of complementary and alternative medicine in patients with inflammatory bowel disease. Gastroenterol Hepatol. 2018 Jul;14(7):415-425. PMID: 30166957; PMCID: PMC6111500
THERESA LOWRY-LEHNEN, RGN, PG Dip Coronary Care, RNP, BSc, MSc, PG Dip Ed (QTS), M Ed, PhD, Clinical Nurse Specialist and Associate Lecturer, South East Technological University











Leave a Reply
You must be logged in to post a comment.