NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Colorectal cancer (CRC) is the third most common cancer globally.4,5 It accounts for approximately 10 per cent of all diagnosed cancers and almost 900,000 cancer-related deaths annually worldwide. The major factor that increases a person’s risk for colorectal cancer is advancing age. While stabilising and decreasing trends are seen in some highly-developed countries, mainly attributed to nationwide screening programmes and increased uptake of colonoscopy, worrying increases in patients younger than 50 years presenting with CRC have been observed, especially with rectal and left-sided colon cancer. Although genetic, environmental and lifestyle factors including decreased physical activity and increased obesity rates have some association, the exact reasons for this increase in people aged under 50 years of age are not completely understood.6 The incidence of CRC globally is predicted to increase to 2.5 million new cases in 2035.1,2
Each year in Ireland approximately 2,800 new cases of CRC are reported (2018-2020).13,15 In 2020, the estimated age-standardised mortality rate of CRC in males in Ireland of 26.5 per 100,000 was 7.7 per cent higher than the EU27 rate of 24.6 per 100,000, while the estimated age-standardised mortality rate in females in Ireland of 15.7 per 100,000 was 12.1 per cent higher than the EU27 rate of 14.0 per 100,000.16 The incidence of CRC in Ireland is projected to rise, and by 2045 the incidence is projected to increase by 114 per cent in females and 129 per cent in males based on demographic changes alone.13,14
A productivity loss analysis carried out in an Irish context (2016) projected that by 2030, premature death because of CRC will cause a value of €237,664 lost household per death and an overall productivity loss per population of €2.5 billion.17
If diagnosed early, CRC has a high five-year survival rate, however, the disease remains a significant cause of mortality. Although curable in its early stages, CRC is largely an asymptomatic disease until it reaches an advanced stage.1 CRC almost always develops slowly over many years from benign growths in the colon or rectum. With appropriate screening, lesions can be identified and removed before they become malignant.6 Colonoscopy remains the gold standard for CRC screening.1,3
About 95 per cent of CRC cases are caused by adenomatous polyps on the epithelial mucosa of the intestinal lining. Polyps can be raised, flat, benign, precancerous, or cancerous. The malignant progression of dysplasia, carcinoma in situ, cancer, and metastasis applies to polyps, and by removing polyps early, progression is interrupted.3
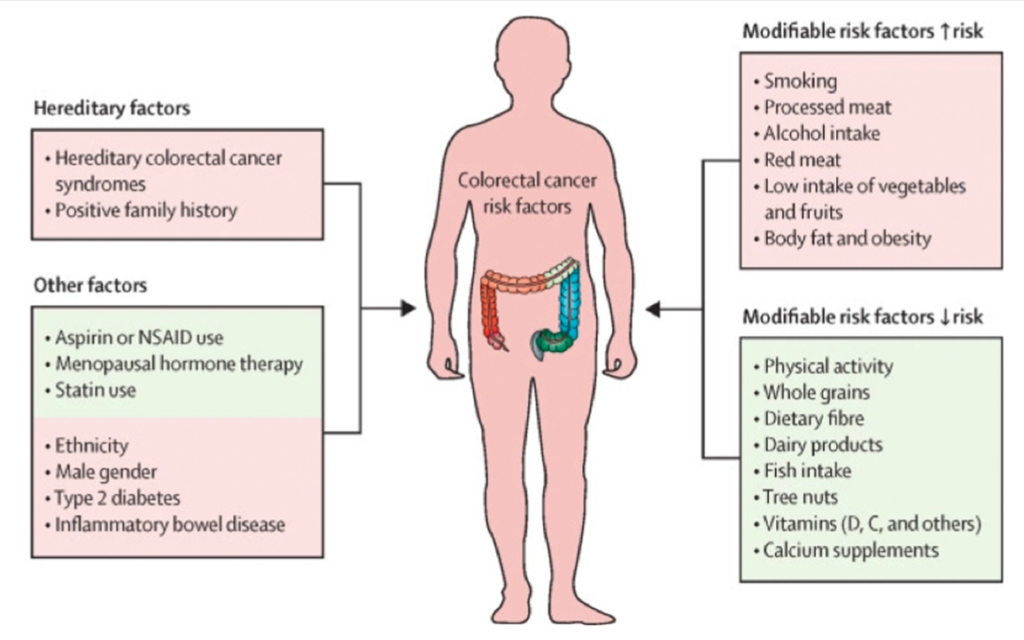
There are multiple risk factors for CRC, often divided into modifiable and non-modifiable risk factors. Non-modifiable risk factors include age, family history, ethnicity, and a personal history of a predisposing genetic syndrome or inflammatory bowel disease. Modifiable risk factors include lack of physical exercise, a diet low in fruits, vegetables, fibre and high in fat, red meat, processed meat, smoking, drinking alcohol, and being overweight or obese.
Risk factors of colorectal cancer include:3,12
Increasing age: More than six-in-10 cases are in people over the age of 65 years. Less than 10 per cent of cases are diagnosed in people under the age of 50 years.
Previous bowel cancer
Family history of bowel cancer: If a member of the immediate family or relatives on the same side of the family has had bowel cancer, or if an immediate family member was diagnosed with bowel cancer at a young age, under 45.
Inherited bowel conditions: FAP (familial adenomatous polyposis) and Lynch syndrome (also called hereditary nonpolyposis colorectal cancer).
Other bowel conditions: A history of a bowel condition such as benign polyps, ulcerative colitis, or Crohn’s disease.
Obesity
Diet: A diet high in fat and red meat and low in fibre, fruit, and vegetables can increase the risk of bowel cancer.
Excess alcohol and smoking may increase the risk for some people.
Screening remains the most important means of preventing CRC. Bowel screening aims to detect signs of bowel cancer at an early stage, where there are no symptoms. BowelScreen is the National Bowel Screening Programme in Ireland, which offers free bowel screening to people aged 60-to-69 years every two years. Over time the BowelScreen programme will be expanded until the full 55-to-74-year age group is reached. BowelScreen sends a letter to people aged 60-to-69 asking them to take part in the bowel screening programme. Men and women who are called for screening and who are willing to take part in the screening programme are sent a home faecal immunochemical test (FIT) in the post. The easy-to-use test kit includes step-by-step instructions for completing the test and sending the samples by Freepost to a laboratory, where the sample will be tested for the presence of blood.7,8 Test results are expected to be normal for more than nine-in-10 people, who will be invited for routine screening again in two years. Approximately five-in-100 people receive an abnormal result and will be referred to hospital for a colonoscopy to determine any abnormality in the bowel.8 BowelScreen can be contacted online (www,bowelscreen.ie) or by Freephone 1800 45 45 55 for people to check if they are on the register.
Uptake of BowelScreen is not optimal and a new study looking into the reasons behind this has uncovered some interesting findings. The Irish research found that people who did not take the home test kit were more likely to react defensively to their bowel screening invitation. Peoples’ defensiveness was in some instances driven by misconceptions they held, such as having a healthy lifestyle or having regular bowel movements. Because of these factors they said they believed they did not need to be screened. Some people believed they could put off doing the screening test until there was a ‘better’ test – even though the current BowelScreen test works well and is the best home bowel screening kit available.
Others said that it was best to delay screening while they sorted out their other health concerns. Another common reason for a defensive reaction to an offer of bowel screening was the belief that cancer is always fatal. The results suggest that screening programmes need strategies to decrease procrastination and address misconceptions about bowel cancer and screening. The study, ‘The role of defensive information processing in population-based colorectal cancer screening uptake’, has recently been published in the journal Cancer.22
Symptoms
Signs and symptoms of CRC include:
A persistent change in bowel habits, including diarrhoea or constipation or a change in the consistency of stool.
Rectal bleeding or blood in stools.
Persistent abdominal discomfort, such as cramps, gas, or pain.
A feeling that the bowel does not empty completely.
Weakness or fatigue.
Unexplained weight loss.
Many people with CRC experience no symptoms in the early stages of the disease. When symptoms appear, they vary, depending on the cancer’s size and location.
Diagnosis
In addition to the patient’s symptoms, medical history and a physical examination including abdominal and digital rectal examination (DRE), other tests may be used to help diagnose CRC and its spread to other areas.9
Sigmoidoscopy;
Colonoscopy;
Biopsy;
Blood tests, including FBC to check for anaemia, LFTs, tumour markers;
Biomarker testing of the tumour;
CT scan;
Ultrasound;
MRI;
CXR;
PET scan.
If signs of CRC are found during a colonoscopy, other tests will follow. A biopsy may be performed, often during the colonoscopy, and analysed for the presence of cancer cells. Once a diagnosis is confirmed by colonoscopy and biopsy, blood tests and imaging tests, such as CT and MRI scans, may be used to learn more about the cancer and whether it has spread.11
The most common type of CRC is adenocarcinoma, which makes up approximately 95 per cent of all CRC cases. In the gastrointestinal tract, rectal and colon adenocarcinomas develop in the cells of the lining inside the large intestine. These adenocarcinomas typically start as a polyp, which may develop into cancer. There are two rare types of adenocarcinomas: Mucinous tumours and signet ring tumours.11
Mucinous adenocarcinoma is made up of about 60 per cent mucus. The mucus may cause cancer cells to spread more quickly and become more aggressive than typical adenocarcinomas. Mucinous adenocarcinomas account for 10-to-15 per cent of all rectal and colon adenocarcinomas.11
Signet ring cell adenocarcinoma accounts for fewer than 1 per cent of all colon cancers. Named after its appearance under a microscope, signet ring cell adenocarcinoma is aggressive and may be more difficult to treat.11
Less common types of CRC include:11
Primary colorectal lymphomas: A type of non-Hodgkin lymphoma, this cancer type develops in the lymphatic system, specifically in the lymphocytes. Primary colorectal lymphomas account for 0.5 per cent of all CRC and about 5 per cent of lymphomas. This CRC type usually develops later in life and is more common in men.11
Gastrointestinal stromal tumours (GISTs) are a rare type of CRC that form in cells found in the lining of the gastrointestinal (GI) tract called interstitial cells of Cajal (ICCs). More than 50 per cent of GISTs develop in the stomach. While most other GISTs form in the small intestine, the rectum is the third most common location. GISTs are classified as sarcomas, or cancers that begin in the connective tissues, which include fat, muscle, blood vessels, deep skin tissues, nerves, bones, and cartilage.11
Leiomyosarcomas are another form of sarcoma. Leiomyosarcoma means ‘cancer of smooth muscle’. The colon and rectum have three layers of the type of muscle affected by leiomyosarcoma and all three work together to guide waste through the digestive tract. This rare type of CRC accounts for about 0.1 per cent of all colorectal cases.11
Carcinoid tumours develop in nerve cells called neuroendocrine cells, which help regulate hormone production. These tumours are among a group of cancers called neuroendocrine tumours (NETS). Carcinoid tumour cells are slow-growing and may develop in the lungs and/or GI tract. They account for about 1 per cent of all CRCs and half of all cancers found in the small intestine.11
Melanomas may start to develop anywhere, including in the colon or rectum, or may spread to the GI tract from the primary melanoma site. Melanomas account for 1-to-3 per cent of all cancers that develop in the digestive system. How melanoma develops in the colon is not well understood, as it is extremely rare.11
Grading: Grades of bowel cancer cells range from 1-to-4.10.
Staging: The stage of a cancer shows how large it is and how far it has spread.10 Bowel cancer staging includes the TNM and number staging systems.
Treatment
As mentioned, guideline-wise there is a National Clinical Guideline: Diagnosis, Staging and Treatment of Patients with Colon Cancer. The European Society for Medical Oncology (ESMO) has also published guidelines on the diagnosis, treatment and follow-up of localised colon cancer (2020), while this year (2023) ESMO published a new guideline for the diagnosis, treatment and follow-up of metastatic colon cancer (available here: www.esmo.org/guidelines/guidelines-by-topic/gastrointestinal-cancers/metastatic-colorectal-cancer).
Main treatments for bowel cancer include surgery, chemotherapy, biological therapy, and radiotherapy. Colon cancer is distinct from rectal cancer, with different aetiologies and risk factors. The treatment for colon cancer can require highly-specialised care and can cause several cancer-specific issues for patients, which require expert management to provide the best outcomes. The diagnosis, staging, and treatment of patients with colon cancer requires multidisciplinary care in an acute hospital setting.13 CRC can impair quality-of-life through direct and indirect consequences of the disease. Each treatment method is associated with specific adverse effects and complications.1
Surgery is the cornerstone of curative treatment and the primary treatment for CRC that is limited to the colon. It aims to remove cancerous tissue, including tumours and affected lymph nodes, and prevent the cancer from spreading. Surgery usually involves removing a section of bowel and re-joining the two ends. Sometimes it is not possible to re-anastomose and the patient may require a stoma (temporary or permanent).18 Surgery for colon cancer may be open, involving a large incision, or laparoscopic. Laparoscopy has become the standard technique for colon cancer in many countries worldwide, with proven short-term benefits in randomised trials and population studies.1
Restoration of bowel continuity can be mostly accomplished in colon cancer but may need a tailored approach in rectal cancer. The closer the anastomosis is to the anus, the higher the risks are and poorer the functional outcome is. Surgery for rectal cancer is more complex related to the accessibility and intricate anatomy of the pelvis. Total mesorectal excision is the standard oncological approach to rectal cancer, and the extent of resection further depends on involvement of the sphincter complex and other surrounding structures. CRC can also present as an emergency with obstruction or perforation. Colonic obstruction can be relieved by a decompressing colostomy or endoscopic stenting, after which staging and patient status can be optimised. Decision for stenting should be multidisciplinary.1
Chemotherapy and radiotherapy may be used, depending on each patient’s situation. Chemotherapy can be given before surgery (neoadjuvant), alongside radiotherapy, or after surgery (adjuvant). Chemotherapy drugs commonly used to treat bowel cancer include: Fluorouracil (5FU), often given with folinic acid; capecitabine, oxaliplatin, and irinotecan. Side-effects to be aware of are cumulative neuropathy including paraesthesia, numbness or tingling affecting activities of daily living, and liver toxicity. Radiotherapy can be neoadjuvant or adjuvant and is used mainly in the treatment of cancer in the rectum and anus.18,19 Radiotherapy can be used before surgery to shrink a tumour so it is easier to remove, and in some cases after surgery to destroy any small amounts of cancer cells that may be left.19
Some biological therapies such as monoclonal antibodies can help some people with advanced CRC to live longer when added to standard chemotherapy treatment. It can also improve the person’s quality-of-life. Biological therapies, such as bevacizumab, cetuximab, and panitumumab, are usually given for advanced CRC along with chemotherapy drugs fluorouracil (FU or 5FU); oxaliplatin; or irinotecan.19
Metastatic disease can give rise to a range of additional symptoms that negatively affect the patient’s quality-of-life. Maintaining optimal nutrient intake and physical condition, with exercise, adequate pain relief, and psychosocial support, can improve quality-of-life.
Prevention
Population growth, demographic ageing, and unfavourable trends in major risk factors, such as physical inactivity, overweight and obesity, smoking, increased alcohol consumption and poor dietary habits, are increasing CRC incidence. CRC shares several main risk factors with other common diseases, and primary prevention efforts to reduce these risk factors can have multiple beneficial effects that extend beyond CRC prevention. Maintaining a healthy weight may help lower the risk. Being more active lowers the risk of CRC and polyps, and increasing the amount and intensity of physical activity may help reduce the risk. Many studies have found a link between the consumption of red and processed meats and increased CRC risk. Diets low in red and processed meats and those which include a good intake of vegetables, fruits, whole grains, fibre, and dairy products have been linked with a decreased risk of colon or rectal cancer. Smoking cessation and reduced alcohol intake can help reduce the risk of CRC.20
Major reductions in the CRC burden are possible through effective secondary prevention. Mortality from CRC can be reduced through screening and detection. A sizeable reduction in the incidence and mortality of CRC can be achieved by offering effective screening tests, such as FIT, flexible sigmoidoscopy, and colonoscopy, in organised screening programmes, which have been implemented in an increasing number of countries.1 The portfolio of non-invasive or minimally invasive screening tests is expected to be expanded in the years to come by the discovery of novel molecular markers, in particular, blood-based ‘omics signatures’.20
There is consistent evidence that aspirin and NSAIDs protect against CRC. Forty-five studies on over 150,000 CRC cases indicate that aspirin use is associated with a greater than 25 per cent risk reduction.
Additional reporting by Priscilla Lynch
References
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019 Oct 19;394(10207):1467-1480
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394-424
Walden P. The facts about colorectal cancer. Nursing Made Incredibly Easy. 2021. Available at: https://journals.lww.com/nursingmadeincrediblyeasy/fulltext/2021/09000/the_facts_about_colorectal_cancer.10.aspx
Husebø AML, Karlsen B, Husebø SE. Health professionals’ perceptions of colorectal cancer patients’ treatment burden and their supportive work to ameliorate the burden – a qualitative study. BMC Health Serv Res. 2020 Jul 17;20(1):661
Tuominen L, Leino-Kilpi H, Meretoja R. Expectations of patients with colorectal cancer towards nursing care – a thematic analysis. Eur J Oncol Nurs. 2020 Feb;44:101699
Simonson C. Colorectal Cancer – An update for primary care nurse practitioners. The Journal for Nurse Practitioners. 2018 Feb;14(4), 344-350
Citizens Information. BowelScreen: The National Bowel Screening Programme. 2023. Available at: www.citizensinformation.ie/en/health/health_services/cancer_services/bowelscreen.html
Irish Cancer Society. Bowel Cancer Screening. 2023. Available at: www.cancer.ie/cancer-information-and-support/cancer-types/bowel-colorectal-cancer/bowel-cancer-screening
HSE. Bowel Cancer: Symptoms and Diagnosis. 2022. Available at: www2.hse.ie/conditions/bowel-cancer/
Cancer Research UK. Bowel Cancer: Stages and Grades. 2023. Available at: www.cancerresearchuk.org/about-cancer/bowel-cancer/stages-types-and-grades/TNM-staging
Markman M. Colorectal Cancer Types. Cancer Centre.com. 2023. Available at: www.cancercenter.com/cancer-types/colorectal-cancer/types
Marie Keating Foundation. Bowel Cancer: What you should know. 2023. Available at: https://mariekeating.ie/cancer-information/bowel-cancer/bowel-cancer-know/
HSE. Diagnosis, staging and treatment of patients with colon cancer: National Clinical Guideline No 24. 2020. Available at: www.hse.ie/eng/services/list/5/cancer/profinfo/guidelines/diagnosis-staging-and-treatment-of-patients-with-colon-cancer.pdf
National Cancer Registry Ireland (NCRI). Cancer incidence projections for Ireland 2020-2045. April 2019. Available at: www.ncri.ie/publications/cancer-trends-and-projections/cancer-incidence-projections-ireland-2020-2045
National Cancer Registry Ireland (NCRI). Cancer in Ireland 1994-2018 with estimates for 2018-2020: Annual report of the National Cancer Registry. December 2020. Available at: www.ncri.ie/publications/statistical-reports/cancer-ireland-19
European Cancer Information System (ECIS). Estimated incidence by country – summary [Online]. 2020. Available at: https://ecis.jrc.ec.europa.eu/
Pearce A, Bradley C, Hanly P, O’Neill C, Thomas AA, Molcho M, Sharp L. Projecting productivity losses for cancer-related mortality 2011-2030. BMC Cancer. 2016 Oct 18;16(1):804
James Hospital, Dublin. Bowel (Colorectal) Cancer. 2023. Available at: www.stjames.ie/cancer/typesofcancer/bowelcolorectalcancer/
Marie Keating Foundation. Treatment for advanced bowel cancer. 2023. Available at: https://mariekeating.ie/cancer-information/bowel-cancer-old-page/treatments-advanced-bowel-cancer/
Brenner H, Chen C. The colorectal cancer epidemic: Challenges and opportunities for primary, secondary, and tertiary prevention. Br J Cancer. 2018 Oct;119(7):785-792
Bosetti C, Santucci C, Gallus S, Martinetti M, La Vecchia C. Aspirin and the risk of colorectal and other digestive tract cancers: an updated meta-analysis through 2019. Ann Oncol. 2020 May;31(5):558-568
Clarke N, Hayes L, McQueen A, Gallagher P, Kearney PM, McNamara D, et al. The role of defensive information processing in population-based colorectal cancer screening uptake. Cancer. 2023 Apr15;129(8):1253-1260












Leave a Reply
You must be logged in to post a comment.