NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
By
Theresa Lowry-Lehnen, Rgn, Gpn, Rnp, Phd
- 23rd Aug 2022
CKD is usually insidious, develops slowly over time, and most people affected are asymptomatic until the disease becomes advanced.
Chronic kidney disease (CKD) is a progressive renal disorder that commonly occurs in the adult population, especially in those with hypertension and diabetes. There is no cure, and the condition is associated with high morbidity and mortality rates.1 Approximately 10 per cent of adults globally are affected by some form of CKD, which results in 1.2 million deaths and 28 million years of life lost annually.2,3 CKD affects an estimated 1:10 people in the whole population, and over 500 people in Ireland develop kidney failure every year.8 By 2040, it is estimated that CKD will become the fifth leading cause of death globally.4
CKD is defined as a reduction in kidney function, with estimated glomerular filtration rate (eGFR) of <60mL/min per 1.73m², or markers of kidney damage, such as albuminuria, haematuria, or abnormalities detected through laboratory testing or imaging, and that are present for at least three months.1
CKD is usually insidious, develops slowly over time, and most people affected are asymptomatic until the disease becomes advanced (eGFR <30mL/min per 1.73 m²).8 The rate of kidney function loss varies by aetiology, exposures, and interventions but, in most cases, progression to kidney failure takes between months and decades to develop. Signs and symptoms of kidney failure result from progressive uraemia, anaemia, volume overload, electrolyte abnormalities, mineral and bone disorders, and acidaemia, and lead to death if left untreated.1 Kidney function can decline gradually over several years, or rapidly over several months. In some people, kidney function can drop so low that dialysis treatment or a kidney transplant will be required; ie, end stage kidney disease (ESKD). 9
For individuals with established CKD, addressing complications, associated comorbidities and managing symptoms in addition to protecting kidney function are important steps. Slowing the progression of CKD can be achieved through a range of lifestyle, dietary, and pharmacological strategies, which include weight loss, moderate dietary protein restriction, blood pressure and glucose control, and renin-angiotensin-aldosterone system blockade. Cardiovascular disease is a leading cause of death in patients with CKD, and is a major focus of preservative care in this population.1
Diabetes, which affects more than 250,000 people in Ireland, is one of the leading causes of CKD. Diabetes Ireland highlights the importance of screening for CKD in diabetes patients. Diabetes check-ups include the routine monitoring of kidney function so that changes can be detected early.8
CKD risk factors and aetiology
Risk factors for CKD include older age (>50 years), low birth weight, obesity, smoking, high blood pressure, diabetes, a family history of kidney disease, being of African-American decent, and long-term use of over the counter medications. Both genomic and environmental factors contribute to this complex heterogeneous disease, and CKD heritability is estimated to be high at 30–75 per cent. There is a higher incidence and prevalence of CKD in women than men, however, women have a lower risk of CKD progression, and men are more likely to develop ESKD.
The most common causes of CKD are diabetes (type 1 and type 2) and hypertension. Other causes include primary glomerulonephritis, chronic tubulointerstitial nephritis; hereditary or cystic diseases, secondary glomerulonephritis or vasculitis and plasma cell dyscrasias or neoplasm. Autoimmune diseases, such as lupus, can damage blood vessels and make antibodies against kidney tissue. In addition to known causes, CKD can also be idiopathic.1,6
CKD may result from disease processes in any of the three categories: prerenal – decreased renal perfusion pressure; intrinsic renal – pathology of the vessels, glomeruli, or tubules and interstitium; or postrenal – obstructive.5 Chronic prerenal disease occurs in patients with chronic heart failure or cirrhosis with persistently decreased renal perfusion, which increases the tendency for multiple episodes of an intrinsic kidney injury, such as acute tubular necrosis (ATN). This leads to progressive loss of renal function over time.5
Intrinsic occurs when direct damage to the kidneys causes a sudden loss in kidney function. The most common chronic renal vascular disease is nephrosclerosis, which causes chronic damage to blood vessels, glomeruli, and tubulo/interstitium. The other renal vascular diseases are renal artery stenosis from atherosclerosis or fibro-muscular dysplasia, which over months or years cause ischaemic nephropathy, characterised by glomerulosclerosis and tubulointerstitial fibrosis.5 Chronic obstruction may be due to prostatic disease, nephrolithiasis or abdominal/pelvic tumour with mass effect on ureter(s). Retroperitoneal fibrosis is a rare cause of chronic ureteral obstruction.5
Signs and symptoms
Kidney disease tends not to cause symptoms at the early stage, therefore routine screening using urine and blood tests is important. Symptoms develop over time and can include weight loss, anorexia, oedema of the ankles, feet and hands, dyspnoea, fatigue, nocturia, haematuria, nausea, headaches, muscle cramps, headaches, and erectile dysfunction in men.7
A thorough medical history, physical examination and investigative tests are required to form a diagnosis for CKD. Early CKD stages are usually asymptomatic, and symptoms manifest in stages 4 or 5. The ICGP has a useful guidance document (Chronic Kidney Disease: Diagnosis and management in primary care) on CKD for GPs.14
CKD is typically identified through routine screening with blood serum chemistry profile (serum creatinine concentration should be measured, allowing calculation of eGFR) and urinalysis (ACR-albumin: creatinine ratio) or as an incidental finding. Urine dipstick is first performed, and is a useful screening tool although it only provides a semi-quantitative assessment of level of proteinuria, as the reported value can vary according to the hydration status of the patient. Spot urine sample is sent to the laboratory to measure protein/albumin to creatinine ratio. This will detect even small levels of proteinuria and is essential for diagnosis, but is not useful for routine follow-up of patients who already have established macroalbuminuria. At the same time, a midstream urine specimen (MSU) should be sent for culture to exclude urinary tract infection. The eGFR is a useful and accurate measure of renal function, and is calculated using serum creatinine as well as the variables of age, gender and race. In the following circumstances, however, eGFR may not be accurate: Acute renal failure; patients less than 18 years of age; patients with advanced muscle wasting and amputations; and pregnancy.14
Less commonly, patients may present with symptoms such as gross haematuria, foamy urine, nocturia, flank pain, or decreased urine output. If CKD is advanced, patients may report fatigue, poor appetite, nausea, vomiting, metallic taste, unintentional weight loss, pruritus, changes in mental status, dyspnoea, or peripheral oedema.12
In assessing a patient, additional symptoms that might suggest a systemic cause such as haemoptysis, rash, lymphadenopathy, hearing loss, neuropathy; or urinary obstruction such as hesitancy, urgency, frequency or incomplete bladder emptying should be enquired about. Patients should be assessed for risk factors of kidney disease including prior exposure to potential nephrotoxins such as non-steroidal anti-inflammatory drugs (NSAIDs); antibiotic therapies such as gentamicin and chemotherapies; history of nephrolithiasis or recurrent urinary tract infections; the presence of comorbidities; family history of kidney disease; and other known genetic risk factors.12
A detailed physical examination may provide additional information regarding the underlying cause of CKD. Signs of volume depletion may reflect poor oral intake, vomiting, diarrhoea, or over diuresis, whereas signs of volume overload may be due to decompensated heart failure, liver failure, or nephrotic syndrome. The presence of arterial-venous nicking or retinopathy on retinal examination suggests long-standing hypertension or diabetes. Patients with carotid or abdominal bruits may have renovascular disease. Flank pain or enlarged kidneys should prompt consideration of obstructive uropathy, nephrolithiasis, pyelonephritis, or polycystic kidney disease. Neuropathy may be due to diabetes or less commonly vasculitis, or amyloidosis. Skin findings may include rash, palpable purpura, telangiectasias, or extensive sclerosis. Patients with advanced CKD may exhibit pallor, skin excoriations, muscle wasting, asterixis, myoclonic jerks, altered mental status, and pericardial rub.12
Other diagnostic investigations carried out may include an ultrasound, MRI or CT scan and a biopsy. Once a diagnosis of CKD has been established, the next step is to determine staging.
Stages and classification of CKD
The stages of CKD range from 1-5. Most patients who are diagnosed as having stage 1, 2 or 3, have mild-to-moderate kidney disease and usually do not progress to ESKD. Once stage 4 is reached, damage is more severe and is usually not reversible. Dialysis or a kidney transplant may be required.9
A patient is considered to have CKD if they have abnormalities of kidney function or structure present for more than three months. The definition of CKD includes all individuals with markers of kidney damage or those with an eGFR of less than 60ml/min/1.73m2 on at least two occasions, 90 days apart with or without markers of kidney damage. Markers of kidney disease may include: Albuminuria (ACR >3mg/mmol), haematuria (presumed or confirmed renal origin), electrolyte abnormalities due to tubular disorders, renal histological abnormalities, structural abnormalities detected by imaging (eg, polycystic kidneys, reflux nephropathy), or a history of kidney transplantation.11
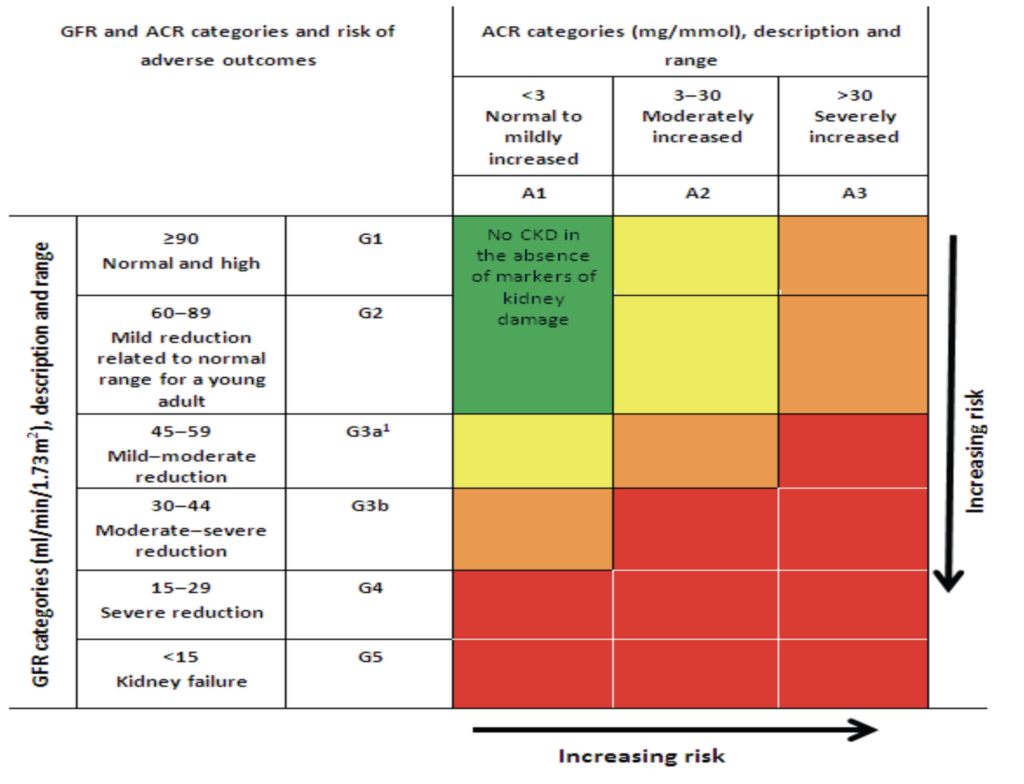
CKD is classified based on the eGFR and the level of proteinuria and helps to risk stratify patients. Patients are classified as G1-G5, based on the eGFR, and A1-A3 based on the ACR albumin: Creatinine ratio.11
CKD stages include:11
G1: GFR 90ml/min per 1.73 m2 and above.
G2: GFR 60 to 89ml/min per 1.73m2.
G3a: GFR 45 to 59ml/min per 1.73m2.
G3b: GFR 30 to 44ml/min per 1.73m2.
G4: GFR 15 to 29ml/min per 1.73m2.
G5: GFR < 15ml/min per 1.73m2 or treatment by dialysis
The three levels of albuminuria include albumin-creatinine ratio (ACR):11
A1: ACR less than 3mg/mmol (normal to mild).
A2: ACR 3 to 30mg/mmol (moderately increased).
A3: ACR greater than 30mg/mmol (severely increased).
Example: A person with an eGFR of 25ml/min/1.73m2 and an ACR of 15mg/mmol has CKD G4A2, and a person with an eGFR of 50ml/min/1.73m2 and an ACR of 35mg/mmol has CKD G3aA3. It is important to note that patients with an eGFR of >60ml/min/1.73m2 should not be classified as having CKD unless they have other markers of kidney disease. GFR category G2 may be over-diagnosed by eGFR because equations used to estimate GFR may give falsely low results in people with near-normal function.11
Treatment and management
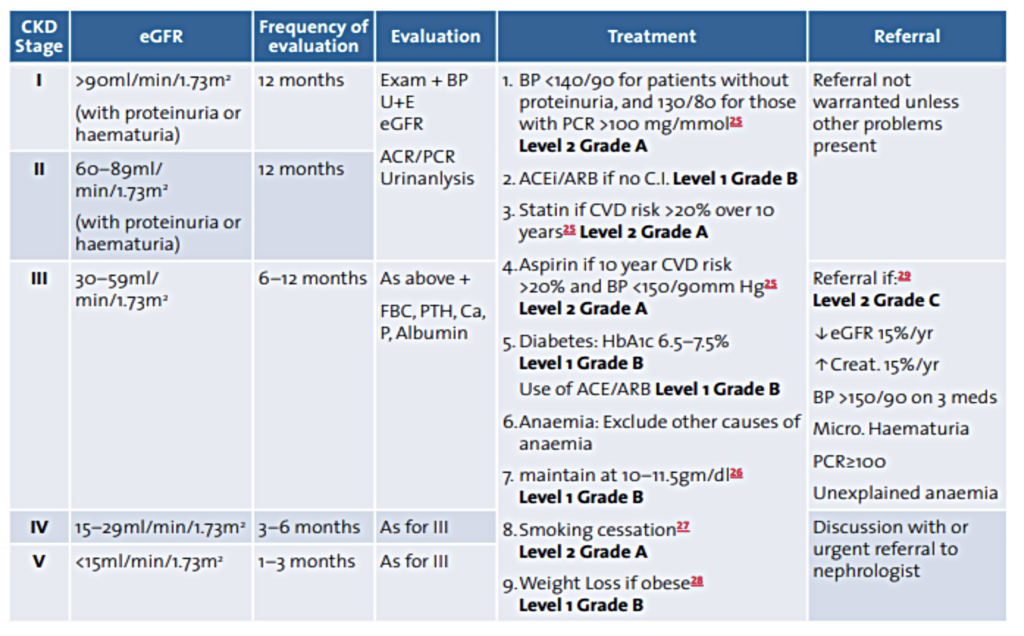
There is no cure for CKD, but treatment and management can help relieve the symptoms and improve the patient’s quality of life. Treatment options and prognosis will depend on the stage of CKD. Lifestyle measures include stopping smoking, a healthy diet, restricted salt intake of less than 6g (<100mmol) per day, regular exercise, manage/ limit alcohol intake, following recommended guidelines, and avoiding over the counter NSAIDs, such as ibuprofen, unless advised by a medical professional.13
The main goals of management of CKD are to reduce overall cardiovascular risk, delay progression to renal failure and avoid complications.14 Regular reviews are recommended and should include blood pressure measurement, assessment of kidney function, review of all medications, and immunisation with influenza vaccine and pneumococcal vaccine, in addition to lifestyle advice regarding smoking, reduced salt intake and weight loss. Anaemia is common in more advanced disease and a target of 10–11.5gm/dL should be sought. If the haemoglobin is low, non-renal causes should be excluded. Management of ‘renal’ anaemia can include the provision of iron and the use of erythropoiesis stimulating agents. Regular review of medication is important to minimise nephrotoxic drugs particularly NSAIDs, and ensure doses of others are appropriate to renal function. Metformin should be avoided in patients with CKD stage G4 and G5.14,15
Risk factors for the development of CKD, such as hypertension and diabetes mellitus, should be specifically targeted. Cardiovascular complications can be reduced by attention to smoking cessation, weight loss, regular aerobic exercise, thrombotic risk, and treatment of hypercholesterolemia. Aspirin treatment should be considered for all patients with an estimated 10-year risk of cardiovascular disease of >20 per cent, so long as blood pressure is <150/90 mmHG.14 Patients with established macrovascular disease should receive treatment for hyperlipidaemia according to the current European Society of Cardiology (ESC) guidelines. Patients with diabetes and CKD but no established macrovascular disease should be offered lipid-lowering drug treatment according to the current ESC guidelines. Patients with CKD who do not have diabetes and who do not have established macrovascular disease should be offered the option of lipid-lowering treatment according to the current ESC guidelines, if the estimated 10-year risk of cardiovascular disease is >20 per cent.14
Management of CKD patients with diabetes mellitus and microalbuminuria or proteinuria include continued efforts to achieve good glycaemic control (HbA1c 6.5–7.5 per cent, 48–58mmols/mol); prescription of an angiotensin-converting enzyme inhibitor (ACEI) (or angiotensin receptor blocker (ARB) in the presence of a firm contraindication to ACEI), titrated to full dose, followed by addition of other antihypertensive drugs in combination to reach the blood pressure goal of 130/80;23 measurement of eGFR and PCR at least once a year; referral to a nephrologist if there is in creasing proteinuria; and consideration of dietary protein restriction for patients with type 1 diabetes.14
Most patients with mild-to-moderate CKD will not require dialysis and can be managed in primary care. Appropriate management of patients in primary care has the potential to reduce overall cardiovascular risk and delay progression to renal failure.
New treatments: The sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin is a promising treatment for certain people with CKD, which has the potential to increase the length of time before the disease worsens. Dapagliflozin was approved in the European Union (EU) in 2021 for the treatment of CKD in adults with and without type-2 diabetes (T2D). Adding dapagliflozin to current standard care in CKD has been shown to significantly reduce the risk of having declining kidney function, ESKD, or dying from causes related to the kidneys or cardiovascular system. In the UK, NICE has recommended dapagliflozin as an option for treating some adults with CKD.16,17 Due to limited experience, it is not recommended to initiate treatment with dapagliflozin in patients with GFR <25mL/min.18
For a small proportion of people with CKD, the kidneys will eventually stop working. This usually happens gradually. Options for people at this stage include dialysis (haemodialysis or peritoneal dialysis), and an alternative to dialysis for people with severely reduced kidney function is a kidney transplant. Transplant is often the most effective treatment for advanced kidney disease, but requires a donor and involves major surgery and the need for immunosuppressant medication for the rest of the patient’s life. Survival rates for kidney transplant patients are very good.13
Help and support
The Irish Kidney Association (IKA) (https://ika.ie/) has been supporting patients with CKD and ESKD in Ireland since 1978. They are dedicated to meeting the needs of patients and their families and carers, living with or likely to be affected by end stage renal disease. The IKA has a network of 25 branches across the country that are supported by volunteers.9
References
1. Kalantar-Zadeh K, Jafar T, Nitsch D, Neuen B, Perkovic V. (2021). Chronic kidney disease. Lancet 398: 786–802. Available at: www.thelancet. com/action/showPdf?pii=S0140-6736%2821%2900519-5
2. Bikbov B, Purcell C, Levey A, et al. (2020). Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2020; 395: 709–33
3. Xie, Y, Bowe B, Mokdad A, et al. (2018). Analysis of the global burden of disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int 2018; 94: 567–81
4. Foreman K, Marquez N, Dolgert A, et al. (2018). Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 2018; 392: 2052–90
5. Vaidya S, Aeddula N. (2021). Chronic renal failure. StatPearls Publishing. Available from: www.ncbi.nlm.nih.gov/books/ NBK535404/
6. Cockwell P, Fisher L. (2020). The global burden of chronic kidney disease. Lancet. 2020; 395: 662-664
7. NHS (2019). Chronic Kidney Disease. National Health Service. Available at: www.nhs.uk/conditions/kidney-disease/symptoms/
8. Mellotte G, Moore C, Clinch T. (2022). Pharmacy supports kidney disease screening. Irish Pharmacy News. Vol 14; Issue 4; pp 26; April 2022
9. IKA. (2022). What is chronic kidney disease? Irish Kidney Association. Available at: https://ika.ie/kidneyhealth/
10. Diabetes Ireland (2022). Diabetes and kidney disease. Available at: www.diabetes.ie/diabetes-and-kidney-disease/
11. UKKA. (2022). CKA Stages. UK Kidney Association. Available at: https://ukkidney.org/health-professionals/information-resources/uk-eckd-guide/ckd-stages
12. Chen T, Knicely D, Grams M. (2019). Chronic kidney disease diagnosis and management: A review. JAMA, 322(13), 1294– 1304. doi:10.1001/jama.2019.14745
13. NHS (2019). Treatment chronic kidney disease.National Health Service. Available at: www.nhs.uk/conditions/kidney-disease/treatment/
14. Glynn L. (2016). Chronic kidney disease: Diagnosis and management in primary care. ICGP. Quality in Practice Committee. Available at: www.icgp.ie/go/library/catalogue/item/73877022- BC62-6AFE-22F01E0145ADCB19/
15. UKKA (2022). CKD Stages G4 and G5. UK Kidney Association. Available at: https://ukkidney.org/health-professionals/ information-resources/uk-eckd-guide/ckd-stages-g4-and-g5
16. NHS (2022). NICE recommend dapagliflozin for people with chronic kidney disease. Available at: www.nice.org.uk/news/ article/nice-recommend-dapagliflozin-for-people-with-chronic-kidney-disease
17. NICE (2021). Chronic kidney disease: Assessment and management. NICE Guideline NG203. Available at: www.nice.org. uk/guidance/ng203
18. Medicines.ie (2021). Forxiga 5mg film-coated tablets/Forxiga 10mg film-coated tablets. Summary of product characteristics last updated on medicines.ie: 22/11/2021. Available at: www. medicines.ie/medicines/forxiga-5-mg-10-mg-film-coated-tablets-34715/spc













Leave a Reply
You must be logged in to post a comment.