NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
The guideline notes that the risk of recurrent venous thromboembolism is increased at least twofold in patients with cancer compared with those without cancer
Venous thromboembolism (VTE) affects at least one-in-20 cancer patients, who are at a fourfold risk of developing thrombosis compared with those who do not have a malignancy.1 Patients who experience cancer-associated thrombosis (CAT) are three times more likely to die than those who do not, and the condition carries substantial additional morbidity, challenges, and psychological and emotional distress.1,2 In some cases, VTE is the first manifestation of malignancy, while others will develop the complication during their cancer trajectory. Several factors contribute to this increased risk of VTE in cancer patients, including tumour type and anatomical factors; age; existing comorbidities; obesity; hospital admission; surgery; immobilisation; the presence of an indwelling central venous catheter (CVC); systemic anti-cancer therapy (SACT); erythropoiesis-stimulating agents; and new molecular-targeted therapies such as antiangiogenic agents.2,3
The British Society for Haematology (BSH) has this year updated its guideline for CAT in adults following a review of key clinical trials and studies by the BSH Haemostasis and Thrombosis Task Force, the BSH Guidelines Committee, and the BSH sounding board.1 The Grading of Recommendations Assessment, Development and Evaluation (GRADE) nomenclature was used to evaluate the evidence level (EL) and to assess the strength of the latest recommendations. The term CAT in the guideline refers to VTE and does not include arterial thromboses.
Thromboprophylaxis
Hospitalised patients: Despite the absence of cancer-specific randomised controlled trials (RCTs) investigating pharmacological thromboprophylaxis in non-surgical hospitalised inpatients, the guideline acknowledges evidence from prospective studies showing that patients hospitalised with an acute medical illness are at increased risk of VTE, that pharmacological thromboprophylaxis reduces the risk, and that several RCTs of thromboprophylaxis with low molecular weight heparin (LMWH) in hospitalised medical patients included participants with cancer.
Surgical prophylaxis: The guideline highlights the well-documented higher risk of VTE in patients with cancer undergoing surgical procedures compared to those without malignancy. Recommendations are based on results from meta-analyses and systematic reviews that reported a reduction in postoperative VTE among cancer patients undergoing surgery that received pharmacological thromboprophylaxis with parenteral anticoagulation.
Ambulatory cancer outpatients: Bleeding risks and other limitations has meant that LMWH thromboprophylaxis in ambulatory cancer outpatients has not been universally adopted, and has led to a focus on trying to identify high-risk oncology patients who would benefit from thromboprophylaxis. This has been done by looking at specific high-risk tumour types, such as pancreatic cancer and multiple myeloma, the use of VTE risk scores, or both in combination with new antithrombotic treatments. According to the guideline, identification of high-risk patients can be aided by the use of cancer-specific VTE risk assessment scores such as the eponymous Khorana score, which predicts thrombosis risk based on tumour type, full blood count result, and body mass index.
Recommendations:
Patients with active cancer admitted to hospital with an acute medical illness should receive pharmacological thromboprophylaxis with LMWH throughout their admission unless contraindicated. (EL: 1A)
Patients with active cancer admitted to hospital for non-minor surgery should receive pharmacological thromboprophylaxis with LMWH throughout their admission unless contraindicated. (EL: 1A)
Thromboprophylaxis should be extended to 28 days postoperatively for high-risk surgical patients, such as those requiring open or laparoscopic surgery for the management of abdominal and pelvic cancer, with LMWH (EL: 1A), or with prophylactic dose rivaroxaban or apixaban after an initial period of LMWH. (EL: 2A)
Myeloma patients should be risk assessed with a myeloma-specific risk assessment score and prophylactic dose anticoagulant offered to those at intermediate or high risk. (EL: 1B)
Pancreatic cancer patients receiving SACT should be offered pharmacological thromboprophylaxis with an anticoagulant in line with the dosage used in clinical trials. (EL: 1B)
Consider assessing other ambulatory patients commencing SACT using a validated risk assessment score for thromboprophylaxis. (EL: 2B)
Consider omitting pharmacological thromboprophylaxis when the platelet count is below 50×109/L. (EL: 2D)
Prevention of catheter-related thrombosis
CVCs are used extensively in managing cancer patients. CVCs, tunnelled lines, subcutaneous ports, and percutaneous inserted central catheters are complicated by symptomatic catheter-related thrombosis (CRT) in 4-to-8 per cent of adult patients, which may adversely affect prognosis and result in serious adverse events including infection, pulmonary embolism, catheter failure, and resultant treatment delays. Evidence to date has been conflicting or sparse to support a gold standard approach.
Recommendation:
Routine use of anticoagulants at prophylactic or therapeutic dose to prevent CRT in cancer patients is not recommended. (EL: 1B)
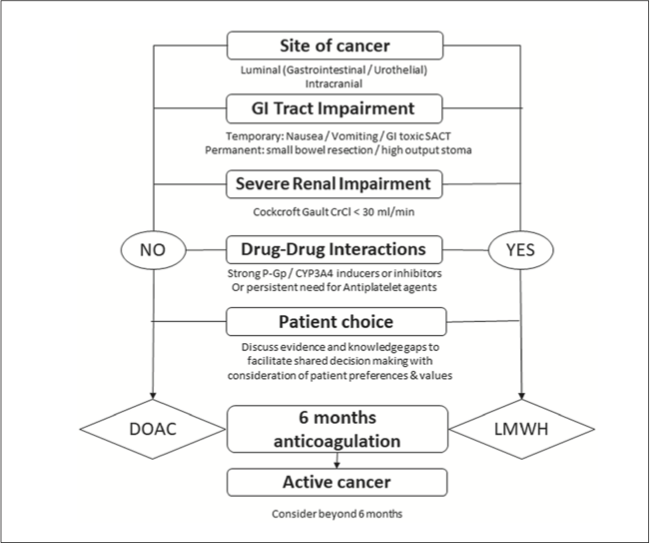
Figure 1: Factors involved in the decision on the most appropriate agent for treatment of CAT
Acute treatment of cancer-associated VTE (up to six months)
The guideline notes that the risk of recurrent VTE is increased at least twofold in patients with cancer compared with those without cancer. It also highlights the increased risk of bleeding in patients with cancer on anticoagulants compared with those without cancer, which complicates the management of this cohort. According to the BSH, estimated fatality from VTE recurrence in the cancer population is greater than that from major bleeding, concluding that there is a benefit from anticoagulation.
Recommendations:
Patients with cancer-associated VTE (other than catheter-related) should be treated with a direct oral factor Xa inhibitor or LMWH for six months initially. (EL: 1A)
Warfarin is a suitable alternative in patients with cancer-associated VTE where anticoagulation is required, but it is not possible to use a direct oral factor Xa inhibitor or LMWH. (EL: 1B)
A shared decision on the most appropriate agent for the treatment of CAT is recommended, and should consider risk of bleeding; tumour site; suitability of oral medications; potential for drug-drug interactions (in particular, strong inhibitors or inducers of CYP-3A4 and P-glycoprotein); and patient preference and values regarding choice of drug. Ongoing assessment of these factors is advised (Figure 1).
Treatment of CRT in cancer patients
The BSH highlights that advances in insertion techniques, catheter material, and ongoing care have resulted in a reduction of symptomatic CRT from around 30 per cent to 5 per cent. There is no evidence to support removal of the catheter if it is functioning, in the correct position, still required for treatment, and exhibiting no evidence of infection.
Recommendation:
Patients with CRT should receive three months of anticoagulation initially, and then continue anticoagulation for as long as the catheter remains in situ. (EL: 2C)
Due to the absence of comparative data, the guideline does not recommend a specific anticoagulant class over another.
Inferior vena cava filters
Evidence supporting the use of inferior vena cava (IVC) filters was deficient during the review.
Recommendations:
Routine use of IVC filters in patients with cancer is not recommended. (EL: 1B)
Consider a temporary IVC filter in patients with acute VTE and a contraindication to anticoagulation or when interruption in anticoagulation is required during the four weeks after diagnosis of acute VTE. (EL: 2C)
Thrombocytopaenia
The presence of thrombocytopenia requires a risk-to-benefit analysis of anticoagulation, according to the guideline. The condition may be a result of the malignancy itself or a side-effect of treatment. The BSH notes that the risk of recurrence is particularly high in the first four-to-six weeks after thrombosis, and although the risk then falls, it can remain high for several weeks or months. Therefore, the benefit of continuing therapeutic anticoagulation needs to be balanced against the risk of bleeding in thrombocytopaenic patients.
Recommendations:
During the acute phase of cancer-associated VTE, if it is not possible to maintain the platelet count above 25×109/L, anticoagulation should be avoided. (EL: 1D)
For patients with acute cancer-associated VTE with a high risk of thrombosis recurrence, consider platelet transfusions to maintain counts above 40-50×109/L and continuation of therapeutic doses of anticoagulation. (EL:2C)
For patients with lower risk of thrombosis recurrence, consider a reduced anticoagulation dose strategy using 50-to-75 per cent or prophylactic-dose LMWH for patients with platelet counts of 25-50×109/L. (EL: 2C)
Treatment of recurrent VTE while on therapeutic anticoagulation
The BSH advocates that patients are specifically asked about concordance with anticoagulation, as a lack of compliance has been identified as a common cause of VTE recurrence.
It also notes that certain types of malignancy, particularly brain, lung, pancreatic, ovarian, or myeloid cancers, as well as the stage and stage progression of the disease have the highest risk for VTE recurrence. Patients with leg paresis are also at higher risk.
Recommendations:
Compliance with treatment and confirmation that the correct anticoagulant dose is being administered should be checked in all patients with recurrent thrombosis. (EL: 1C)
In patients with cancer-associated VTE who develop a recurrence while on therapeutic LMWH or therapeutic direct oral anticoagulent, consider using a supratherapeutic dose of 120-to-125 per cent LMWH, with subsequent treatment guided by the clinical response. (EL:2C)
Alikhan R, Gomez K, Maraveyas A, et al. Cancer-associated venous thrombosis in adults (second edition): A British Society for Haematology Guideline. Br J Haematol. 2024;205(1):71-87
Abu Zaanona MI, Mantha S. Cancer-associated thrombosis. In: StatPearls [Internet]. Treasure Island: StatPearls Publishing; 2024. Available at: www.ncbi.nlm.nih.gov/books/NBK562222/
Elyamany G, Alzahrani AM, Bukhary E. Cancer-associated thrombosis: An overview. Clin Med Insights Oncol. 2014;8:129-137











Leave a Reply
You must be logged in to post a comment.