NOTE: By submitting this form and registering with us, you are providing us with permission to store your personal data and the record of your registration. In addition, registration with the Medical Independent includes granting consent for the delivery of that additional professional content and targeted ads, and the cookies required to deliver same. View our Privacy Policy and Cookie Notice for further details.
Allergic rhinitis and asthma – the united airway disease
By
Ruth Morrow
- 18th Feb 2024
A look at the relationship between allergic rhinitis and asthma, and the latest treatment approaches
Asthma is characterised by variable respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough, and variable expiratory airflow limitation. It is usually associated with airway inflammation (GINA, 2022).1 The exact cause of asthma remains unknown. Numerous triggers can cause symptoms, and these differ from person-to-person. As spring and summer emerges, this can be a challenging time as various pollen levels start to increase.
Allergic rhinitis
It is estimated that over 80 per cent of people with asthma have allergic rhinitis (AR). AR is also a risk factor for asthma with 10-to-40 per cent of people who have AR also having asthma. AR is more likely to develop initially with asthma developing later. Therefore, people with AR should be assessed for asthma due to the increased risk of developing asthma. Similarly, patients with persistent asthma should be assessed for AR.
Symptoms of AR
Typical symptoms of seasonal (hay fever) and perennial AR are:
Sneezing;
Itchy, blocked, or runny nose;
Red, itchy, or watery eyes;
Itchy throat, inner ear, or mouth;
Postnasal drip;
Headaches;
Loss of concentration and generally feeling unwell;
Reduced sensation of taste and smell.
Patients may experience all or some of the above. Symptoms may be confused with symptoms of Covid-19.
The term ‘united airway disease’ or ‘one airway disease’ is opportune, as both rhinitis and asthma are chronic inflammatory diseases affecting both the upper and lower airways. Both conditions can be triggered by allergic or non-allergic triggers and present several phenotypes. Assessment and management of AR and asthma should be jointly carried out, leading to better control of both conditions.
Classification
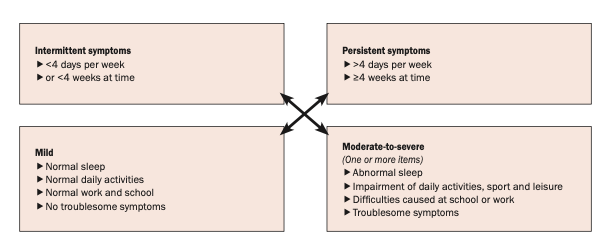
In 2019, the classification of ‘seasonal’ and ‘perennial’ rhinitis was changed to ‘intermittent’ and ‘perennial’ rhinitis (ARIA, 2019).2 Intermittent rhinitis occurs less than four days per week or for less than four weeks. Persistent rhinitis lasts more than four days and longer than four weeks. Both intermittent and persistent AR can be mild or moderate/severe (see Figure 1).
Figure 1: Classification of allergic rhinitis (ARIA, 2019)2
Pharmacological interventions
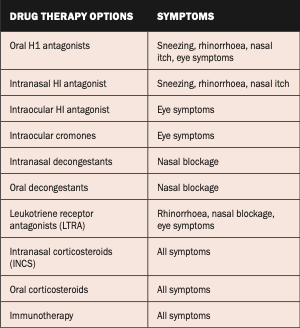
There are several treatment options available to the patient and a combination of these options may be required for optimal relief of symptoms. These are outlined in Table 1.
Table 1: Pharmacological options for the treatment of AR
Saline douching/nasal irrigation should also be encouraged and is available either as a saline rinse or saline spray. Saline rinsing involves high volume at a low pressure, whereas saline spray is a low volume delivered at high pressure. The advantages of saline douching include:
Direct cleansing;
Removal of mucous and inflammatory mediators;
Reduces bacterial burden;
Reduces mucus thickness;
Improves mucociliary function by increasing ciliary beat frequency.
Using a nasal spray
If the nasal spray is being used for the first time, priming is required;
Blow the nose prior to use;
Tilt the head forward;
Use right hand to left nostril, left hand to right nostril;
Aim the nozzle of the spray away from the nasal septum and towards the outer aspect of the nose;
Avoid sniffing deeply;
If the nasal spray can be tasted, the patient is probably sniffing too deeply;
Repeat if a second dose is required;
Repeat the procedure on the other nostril;
Wipe the nozzle of the spray with a tissue before replacing the cap.
Smoking cessation should be encouraged at every opportunity. Smoking increases the likelihood of chronic nasal symptoms and may be associated with the development of nasal polyposis. Passive smoking, environmental exposure, e-cigarettes, and vaping also increase the likelihood of chronic nasal symptoms and nasal polyposis.
Mild intermittent AR treatment options include oral and nasal decongestants, which can be used as a rescue medication. These medications will reduce nasal congestion and should be used for no longer than seven days and should be avoided in pregnancy and breastfeeding. Oral H1 antagonists block the physiological effects from mast cell-derived histamine. Second-generation antihistamines are preferred due to their less sedating effect and are available over the counter. Antihistamines are also available intranasally or intraocular.
Intranasal corticosteroid (INCS) is the first-line treatment for moderate/severe intermittent and persistent AR. These medications are used once- or twice-daily in each nostril and good technique is essential and should be checked at every opportunity. If the nasal cavity is very obstructed, a nasal spray may not be effective. Nasal drops may be more effective in this scenario. Nasal spray technique can be viewed online via Asthma + Lung UK at www.youtube.com/watch?v=S31maomo1xQ. The efficacy of INCS is not improved when used with oral corticosteroids (OCS).
Immunotherapy
Sublingual immunotherapy (SLIT)/allergen immunotherapy (AIT) is now recommended by GINA (2021) as a treatment option for patients with asthma who are sensitised and have AR. Immunotherapy is also recommended by ARIA (2019) for patients with AR who do not achieve an optimal response from oral H1 or INCS therapies. These medications, which are not available on the GMS, can be prescribed by GPs. There are three SLIT/AIT products available in Ireland to treat allergy – grass pollen, tree pollen, and house dust mite allergy.
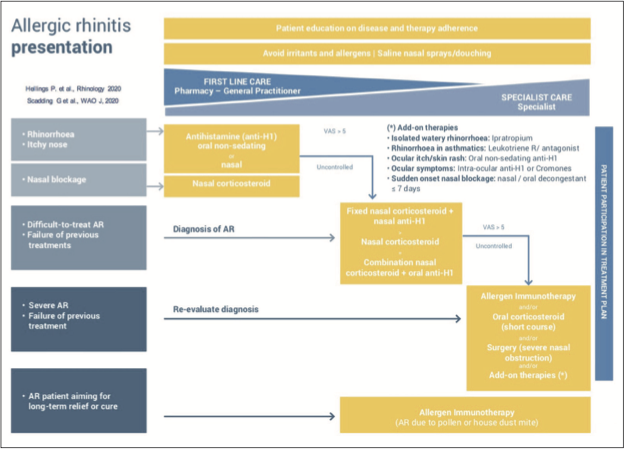
Figure 2 provides a stepwise approach to the management of AR.
Figure 2: Treatment algorithm for AR (Hellings 2020,3 Scadding 20204)
Endonasal phototherapy
Endonasal phototherapy has an immunosuppressive effect by inhibiting allergen-induced histamine released from mast cells. It also induces apoptosis in the T-lymphocytes and eosinophils. The procedure directs a combination of UV-B, UV-A, and visible light into the nasal cavity. Endonasal phototherapy is generally well-tolerated and effective, and is a treatment option when pharmacological treatment is insufficient or contraindicated.
Surgical intervention
It is considered that AR is a medical condition that requires medical intervention. However, if symptoms are unilateral or if there is a septal deviation, nasal polyps, or tumour present, surgery should be considered. Patients will still need to have an AR plan in place post-surgical intervention.
Lifestyle intervention
Keep windows closed at night-time or when the pollen count is high.
Monitor the pollen levels on www.met.ie/forecasts/pollen and minimise time spent outdoors when the pollen count is high.
Apply Vaseline around the nostrils when outdoors to trap pollen.
Wear wraparound sunglasses to minimise levels of pollen irritating the eyes. Splash the eyes with cold water to help flush out pollen and soothe and cool the eyes.
Shower, wash your hair, and change clothes if you have been outdoors for an extended time.
Exercise in the morning rather than the evening when there are higher rates of pollen falling.
Avoid drying clothes outdoors and shake clothes outside before bringing them inside – particularly bedclothes.
Minimise contact with pets that have been outdoors and are likely to carry pollen.
Put an asthma action plan in place. An asthma action plan contains all the information a person with asthma needs to keep their condition in control. Every person with asthma should be offered a plan. It should be reviewed frequently, and any time medication is changed. These can be downloaded from www.asthma.ie and should be filled out with the patient’s healthcare professional.
Exam time
Walker et al (2007)5 showed that AR can have a significant impact on exam performance and results, with students dropping a grade in the State exams compared with their mock exams. Students should be advised to have their AR assessed and treatment started well in advance of sitting exams, usually around Easter time. Some other useful tips during exam time include:
Use non-sedating antihistamines;
Students should tell the adjudicator if their seasonal AR is bothering them;
Splash the eyes with cold water before going into the exam room;
Try not to sit near an open window;
Keep a supply of tissues and effective, quick-acting treatments close at hand, just in case.
Special considerations in AR Children under four years
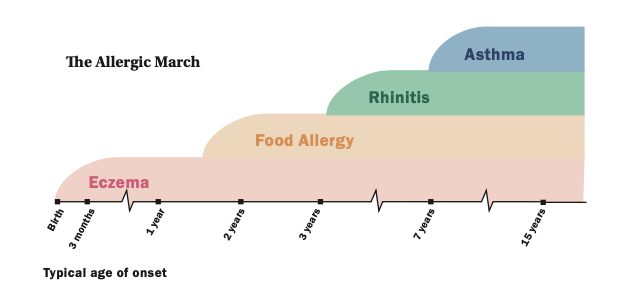
Figure 3 illustrates the typical age of onset of allergies in children. Outdoor allergens are unusual in children under two years of age. Type 2 sub-endotype IL4/IL-13 is associated with AR in children. IL-5 is associated with asthma.
Figure 3: The allergic march in children
Treatment of children aged under four years should focus on allergen avoidance and saline spray. Cetirizine is the oral H1 antagonist of choice. Cetirizine is licensed from two years, but good safety is reported from six months of age. For moderate/severe persistent AR, intranasal corticosteroids such as Fluticasone or Mometasone should be considered first-line treatment. Long-term follow-up studies suggest no growth retardation if used as a once-daily dose. Caution should be taken in children who are also using inhaled or topical corticosteroids for asthma or dermatitis. In children with resistant symptoms and those with co-existing asthma, LTRA should be considered. Parents should be educated about possible side-effects of sleep disturbance and mood disorders.
Pregnancy
AR affects 20 per cent of pregnancies and women with pre-existing AR can experience an increase in symptoms. Medications should be avoided where possible and should only be used if benefits to the mother are greater than the risk to the foetus. Medication should be avoided in the first trimester if possible. Topical administration of medication should be the first-line where possible.
Conclusion
This article has explored the relationship between asthma and AR. Pharmacological and non-pharmacological interventions for the management of AR have been discussed. Special considerations in children and pregnancy have also been addressed.
The impact of AR on health and wellbeing is significant, with many people experiencing impairment of daily activities, learning and cognitive function, as well as reduced productivity at work and school. Optimal control of symptoms through pharmacological and non-pharmacological treatment regimens in combination with education, self-management, and empowerment is paramount to managing this distressing condition.
References
Global Initiative for Asthma (GINA). 2022. Global strategy management and prevention. Available at: www.ginasthma.org
Bousquet JJ, Schünemann HJ, Togias A, Erhola M, Hellings PW, Zuberbier T, et al; ARIA Study Group; MASK Study Group. Next-generation ARIA care pathways for rhinitis and asthma: A model for multimorbid chronic diseases. Clin Transl Allergy. 2019 Sep 9;9:44
Hellings PW, Scadding G, Bachert C, Bjermer L, Canonica GW, Cardell LO, et al. EUFOREA treatment algorithm for allergic rhinitis. Rhinology. 2020 Dec 1;58(6):618-622
Scadding GK, Hellings PW, Bachert C, Bjermer L, Diamant Z, Gevaert P, et al. Allergic respiratory disease care in the Covid-19 era: A EUFOREA statement. World Allergy Organ J. 2020 May 16;13(5):100124
Walker S, Khan-Wasti S, Fletcher M, Cullinan P, Harris J, Sheikh A. Seasonal allergic rhinitis is associated with a detrimental effect on examination performance in United Kingdom teenagers: Case-control study. J Allergy Clin Immunol. 2007 Aug;120(2):381-7
Ruth Morrow, Registered Advanced Nurse Practitioner (Primary Care), Respiratory Nurse Specialist (WhatsApp Messaging Service Asthma Society of Ireland), and Nurse Educator and Consultant












Leave a Reply
You must be logged in to post a comment.